All published articles of this journal are available on ScienceDirect.

A Randomized Controlled Trial: Effectiveness of Smartphone Applications as a Reminder for Improving Oral Hygiene Compliance in Patients Undergoing Orthodontic Treatment
Authors Info & Affiliations
Abstract
Introduction
Maintaining optimal oral hygiene during orthodontic treatment is critical to preventing plaque accumulation, gingivitis, and other periodontal complications. Mobile applications have emerged as potential tools to promote oral hygiene compliance. This Randomized Controlled Trial (RCT) aimed to investigate the effectiveness of a mobile application–based intervention in improving oral hygiene compliance among patients undergoing fixed orthodontic treatment.
Methods
A parallel randomized controlled trial with a 1:1 allocation ratio was conducted among 60 orthodontic patients at Umm Al-Qura University. Participants were randomly allocated into two groups: a control group (n=30) receiving standard oral hygiene instructions, and an intervention group (n=30) receiving the same instructions plus reminders via two smartphone applications: Brushout and Brush teeth reminder. Plaque Index (PI) and Gingival Index (GI) were measured at baseline and after four weeks for both groups. This trial was retrospectively registered on a public online clinical trials registry (www.clinicaltrials.gov) with registration number (NCT06811688), dated 5th February 2025.
Results
Both groups exhibited significant reductions in PI and GI scores after 4 weeks. In the control group, the baseline median PI and GI were 0.42 and 0.27, respectively, while at follow-up, the median PI and GI were 0.25 and 0.1, respectively. For the intervention group, the baseline median PI and GI were 0.43 and 0.25, respectively, while at follow-up, the median PI and GI were 0.2 and 0.08, respectively. However, no significant difference was observed between the intervention and control groups in terms of PI (p = 0.86) and GI (p = 0.38) at follow-up.
Discussion
The findings of the current study contradict previous studies that reported the effectiveness of smartphone applications in improving oral hygiene compliance among orthodontic patients. This discrepancy may be related to several factors, such as user engagement with the application, readiness for behavior change, sample size, follow-up duration, geographical location, and cultural factors. Future research should consider including a larger and more diverse sample, extending the follow-up period, and using applications with interactive elements to better support behavior change.
Conclusion
While both mobile applications and standard verbal instructions improved oral hygiene, using smartphone reminder applications did not lead to better outcomes. Recommendations for future studies include extending the follow-up period and enhancing application features.
Clinical Trial Registration Number
The study was retrospectively registered on a public online clinical trials registry (www. clinicaltrials.gov) under registration number NCT06811688, dated 5th February 2025.
1. INTRODUCTION
In the modern world, smartphones have become essential tools in various aspects of daily life, including healthcare. Numerous mobile applications have been developed to support prevention, diagnosis, monitoring, treatment, and adherence to health interventions [1]. A systematic review of five studies reported short-term improvements in oral hygiene among orthodontic patients who used mobile health applications [2].
Orthodontic appliances can lead to both quantitative and qualitative changes in the oral microbiota, increasing the risk of oral diseases. This necessitates effective risk management to avoid compromising the outcome of orthodontic treatment. Adverse outcomes, such as prolonged treatment duration, plaque accumulation, gingival inflammation, and bleeding gums, can ultimately result in the deterioration of periodontal health [3, 4].
Therefore, it is essential to enhance oral hygiene compliance in orthodontic patients using approaches guided by behavioral theories [5]. Behavioral research has paid significant attention to the impact of smartphone applications on improving oral hygiene adherence in orthodontic populations [2].
The aim of this Randomized Controlled Trial (RCT) was to evaluate the effectiveness of a mobile application used as an active reminder to improve oral hygiene compliance in patients undergoing fixed orthodontic treatment.
2. METHODS
2.1. Study Design
This study was approved by the Umm Al-Qura University Biomedical Research Ethics Committee (Approval No. HAPO-02-K-012-2023-02-1459) and was retrospectively registered on a public online clinical trials registry (www.clinicaltrials.gov) under registration number NCT06811688, dated 5th February 2025. This was a parallel Randomized Controlled Trial (RCT) with two groups and a 1:1 allocation ratio. Subjects were recruited from the orthodontic clinics at the Dental Teaching Hospital of Umm Al-Qura University from 14th of February until the end of July 2023. Written informed consent was obtained from all patients after the study information was explained to them. A simple computer-generated randomization technique was used to allocate each participant to one of two groups. The inclusion criteria were: (1) patients undergoing orthodontic treatment with fixed appliances, and (2) ownership of a smartphone capable of downloading the Brushout app and the Brush Teeth Reminder app. There were no restrictions regarding age or gender. The exclusion criteria were: (1) patients with removable orthodontic appliances and (2) patients who do not own or use smartphones.
2.2. Study Groups
2.2.1. Group I (control)
Participants received only verbal instructions on oral hygiene, including brushing with a soft-bristled toothbrush for 2 minutes, flossing once daily, using a fluoridated oral rinse, caring for orthodontic appliances, and avoiding hard and sticky foods. These instructions were given at the baseline visit, and subjects were re-examined after 4 weeks.
2.2.2. Group II (intervention)
Participants received the same oral hygiene instructions as the control group, with the addition of downloading two mobile applications, Brushout and Brush Teeth Reminder. These applications were selected because they feature twice-daily notifications (morning and night) to remind users to practice oral hygiene. Additionally, oral hygiene practices were tracked through a link sent electronically and monitored by the study researchers as part of the compliance protocol. Like the control group, intervention subjects were re-examined after 4 weeks.
2.3. Primary Outcomes
Two primary outcomes were assessed using the Plaque Index (PI) and Gingival Index (GI), as described by the Silness-Löe plaque index [6]. Six teeth (#16, #12, #24, #36, #32, and #44) were used to evaluate plaque presence on all surfaces: facial, lingual, mesial, and distal. The thickness of plaque was scored as follows: 0 – absence of microbial plaque; 1 – thin film of microbial plaque along the free gingival margin; 2 – moderate accumulation with plaque in the sulcus; 3 – large amount of plaque in the sulcus or pocket along the free gingival margin. The Gingival Index was used to evaluate the condition of the gingiva on the same surfaces. Scoring was as follows: 0 – normal gingiva; 1 – mild inflammation (slight change in color, slight edema, and no bleeding on probing); 2 – moderate inflammation (redness, edema, glazing, and bleeding on probing); 3 – severe inflammation (marked redness and edema with a tendency for spontaneous bleeding or ulceration).
2.4. Blinding and Reliability
Outcome assessors for PI and GI were blinded to the intervention, making this a single-blinded study. Two examiners were calibrated for outcome assessment using ten subjects who were not included in the study.
2.5. Power and Sample Size Calculation
Power and sample size calculations were conducted based on means (0.67 and 0.99) and SD (0.31 and 0.52) for the control and intervention groups, respectively, extracted from the study by Alkadhi et al. Using 80% power and a 5% alpha error, the required sample size was determined to be 30 subjects per group.
2.6. Statistical Analysis
Descriptive statistics included means with standard deviations or medians with Interquartile Ranges (IQR), as well as frequencies with percentages. Nonparametric statistical tests were used due to the ordinal nature of the outcome variables to compare plaque and gingival indices between the groups (Mann-Whitney U test) and within the groups (Wilcoxon matched-pair signed rank test). The experimental and control groups were compared for age using a two-sample independent t-test and for gender using the chi-square test. Statistical analyses were conducted using complete case analysis, meaning missing data were not considered. The Intraclass Correlation Coefficient (ICC) was used to assess calibration between outcome assessors. All statistical analyses, including power and sample size calculations, were performed using STATA software (StataCorp LP, College Station, Texas, USA). A p-value of 0.05 or less was considered statistically significant.
3. RESULTS
The intraclass correlation coefficient (ICC) was greater than 90% for both intra- and inter-examiner calibration of the two examiners assessing the plaque and gingival indices. About 60 subjects were randomly and evenly allocated to the intervention and control groups. All subjects completed the follow-up examination, and none missed their 4-week plaque and gingival measurements, as shown in Fig. (1).
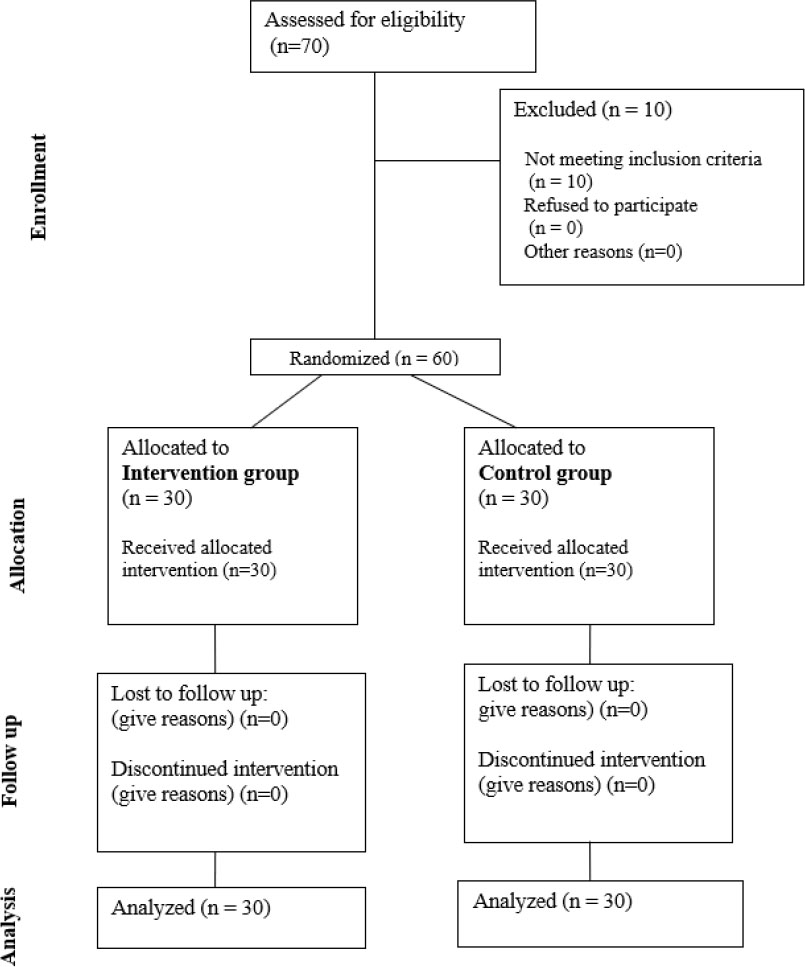
Flow chart of the participants.
| - | Groups | Baseline | Follow-up | p-value ¥ |
|---|---|---|---|---|
| Plaque index | Control (n=30) | 0.42 (0.18-0.91) | 0.25 (0.12-0.41) | 0.0189 |
| Intervention (n=30) | 0.43 (0.33-0.95) | 0.20 (0.12-0.54) | 0.0010 | |
| p-value* | 0.6148 | 0.8646 | - | |
| Gingival index | Control (n=30) | 0.27 (0.08-0.6) | 0.10 (0-0.2) | 0.0179 |
| Intervention (n=30) | 0.25 (0.08-0.66) | 0.08 (0-0.25) | 0.0197 | |
| p-value* | 0.8297 | 0.3785 | - |
The mean age (standard deviation, SD) was 18.6 (3.64) years in the intervention group and 17.57 (4.14) years in the control group, with no significant difference between them (p = 0.31). In the control group, 17 (56.66%) subjects were female and 13 (43.33%) were male. In the intervention group, 19 (63.33%) subjects were female and 11 (36.66%) were male, with p-value 0.598.
There was a significant decrease in PI and GI for both experimental and control groups. Both groups showed a significant decrease in PI and GI. In the control group, the median PI decreased from 0.42 (IQR: 0.18–0.91) to 0.25 (IQR: 0.12–0.41), p = 0.0189. The median GI also decreased significantly from 0.27 (IQR: 0.08–0.6) to 0.10 (IQR: 0–0.2), p = 0.0179 (Table 1). When comparing between experimental and control groups at the follow-up, there was no significant difference in PI, with P = 0.86 and GI. P = 0.38, as shown in Table 1.
4. DISCUSSION
This study aimed to assess the effectiveness of smartphone applications as active reminders for improving oral hygiene compliance in patients undergoing fixed appliance orthodontic treatment. A Randomized Controlled Trial (RCT) design was used, with the control group receiving verbal oral hygiene instructions, while the intervention group received the same instructions plus reminders via smartphone applications. The applications were set to remind patients to brush their teeth twice daily. The GI and PI of patients were assessed at baseline and at a 4-week follow-up. Both groups showed a significant reduction in PI and GI; however, no significant difference was found between the groups. The applications used in this study were chosen to fulfill the primary objective of delivering reminders to participants. Therefore, these findings may be applicable to other applications that provide similar reminder functions.
Several studies have found that using various smartphone applications is effective in improving patients’ behavior and compliance with oral hygiene [7-9]. These studies reported significant differences in plaque and gingival indices between control and intervention groups, as well as a reduction in dental plaque compared to participants who received usual care [7-9]. Moreover, multiple studies [10-13] have demonstrated the effectiveness of text message reminders in improving PI and GI and reducing white spot lesions.
On the other hand, several studies reported no statistically significant effect of smartphone applications on improving oral hygiene in intervention groups [14, 15]. Similarly, Deleuse et al. [16] found no significant improvement in oral hygiene compliance when using an electric toothbrush connected to an application. These findings align with the results of the current study, which showed no significant effect of reminder applications in improving patient compliance with oral hygiene.
Several factors could have resulted in the discrepancies between the findings of our study and previous studies. These include user engagement with the application, readiness for behavior change, sample size, follow-up period, geographical locations, and cultural factors. The applications used in this study lacked features that could have provided sustainable usage, such as gamification, real-time feedback, or behaviorally tailored messages. Previous studies have shown that these features enhance the effect of digital health interventions [9].
Future research should consider utilizing applications that incorporate interactive elements to better support behavioral change. Moreover, users’ readiness for behavior change is strongly correlated with the success of smartphone applications as health interventions [17, 18]. Additionally, variations in geographical and cultural contexts across studies may also influence the outcomes [19, 20].
The main strength of this study was the RCT design. However, several limitations should be considered. First, the follow-up period was relatively short, limiting the ability to assess the long-term effects of smartphone reminders on oral hygiene compliance. Therefore, the findings should be interpreted with caution, as the short follow-up may affect the generalizability of results over a longer timeframe. Future studies with longer follow-up periods, six months or more, are needed to validate these findings.
Second, the study relied on self-reports of oral hygiene behavior, which may be subject to social desirability bias and might not accurately reflect actual behavior. However, clinical assessments using PI and GI at follow-up were conducted to verify compliance. Nevertheless, incorporating app-based analytics, such as login frequency, interaction logs, or brushing sensor data, would offer more reliable and objective verification of compliance with oral hygiene.
Third, the study did not account for potential confounding factors, such as participants’ socioeconomic status, educational background, or level of motivation. These factors could influence oral hygiene behaviors and may have impacted the results. Future studies should include and adjust for these variables to minimize confounding and improve the generalizability of findings.
Additionally, despite the lack of statistically significant differences between groups, the significant improvements in PI and GI within each group should not be overlooked. Future research should investigate the Minimal Clinically Important Differences (MCIDs) for these indices to better inform clinical decision-making [21].
Lastly, although power calculations were performed, the relatively small sample size may limit the generalizability of the findings. Including larger and more diverse populations in future trials will improve external validity and the applicability of results across wider settings.
CONCLUSION
In-office standard verbal, oral hygiene instructions resulted in improved oral hygiene measures for patients undergoing orthodontic treatment. The addition of mobile application-based reminders did not seem to improve oral hygiene outcomes. Further research with larger sample sizes and longer follow-up periods is warranted to explore the potential benefits of mobile applications in improving oral hygiene compliance among orthodontic patients.
AUTHORS’ CONTRIBUTIONS
The authors confirm their contributions to the paper as follows: A.M.: Study conception and design; A.B.S., O.B., S.S., and R.M.: Data collection; S.S. and S.T.: Draft manuscript. All authors reviewed the results and approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| RCT | = Randomized controlled trial |
| PI | = Plaque Index |
| GI | = Gingival Index |
| IQR | = Interquartile range |
| SD | = Standard deviation |
| ICC | = Intraclass correlation coefficient |
| MCIDs | = Minimal clinically important differences |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
This study was approved by the Umm Al-Qura University Biomedical Research Ethics Committee with an approval number (HAPO-02-K-012-2023-02-1459) dated 13th of February, 2023.
HUMAN AND ANIMAL RIGHTS
All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committee and with the 1975 Declaration of Helsinki, as revised in 2013.
AVAILABILITY OF DATA AND MATERIALS
The data that support the findings of this study are available from the corresponding author, [S.S], upon reasonable request.
ACKNOWLEDGEMENTS
Declared none.

