All published articles of this journal are available on ScienceDirect.

The Knowledge and Competence of Dental Practitioners towards Light Curing Units in the Western Region of Saudi Arabia
Authors Info & Affiliations
Abstract
Introduction
The objective of the study is to assess the level of light-curing unit (LCU) knowledge and clinical practice held by dental professionals working in the Western Region of Saudi Arabia.
Methods
The study used a cross-sectional design with an online questionnaire distributed among dental practitioners in the Western Region of Saudi Arabia (n=379). The questionnaire included knowledge of LCUs and material science, clinical practice related to LCUs, maintenance of LCUs, and the level of satisfaction. Descriptive statistics and Pearson's chi-squared test were used for statistical analysis.
Results
Low level of knowledge was reported among participants with significant associations among different specialties, education level, and years of experience (p<0.05). Most participants reported acceptable clinical practice but below-standard maintenance and control of LCUs.
Discussion
Knowledge of LCUs was generally insufficient, with higher levels observed among specialists and those with advanced qualifications. However, the findings may be influenced by the sample's limited geographic diversity and predominance of less experienced general practitioners.
Conclusion
Within the limitations of the study, dental practitioners in the Western Region of Saudi Arabia demonstrated inadequate knowledge and improper maintenance of LCUs despite their acceptable clinical practice of LCUs. This could impact the longevity of the delivered restorations.
1. INTRODUCTION
Conservative dentistry has become an increasingly popular approach in modern dental care with the advancements in adhesive materials. Light curing is a crucial step in many adhesive dentistry procedures, ensuring that the restorative materials achieve their optimal properties for long-term successful restorations [1-3]. Resin-based composite (RBC) have increasingly replaced amalgam and glass ionomer as the preferred material due to their superior esthetics, enhanced bond strength, and improved durability. Nowadays, composite restorations are routinely used in daily dental practice, providing a more conservative approach while meeting both functional and esthetics needs of patients.
The polymerization of RBC restoration is a dynamic process influenced by various factors related to the restorative material, light curing unit (LCU) and its clinical application [1, 4]. The dentist should set the LCU to the appropriate curing mode with sufficient radiant emittance at a specific wavelength that matches the absorption spectrum of the material to cure the RBCs properly [1, 5, 6]. Additionally, the polymerization of RBC is influenced by the shade and thickness of the cured increment, the distance between the light tip and the restoration, and the curing time [4, 7, 8].
Improper polymerization can result in inferior mechanical properties of the restoration, lower bond strength and early failure of the delivered treatment [6, 9, 10]. Thus, efficient light curing units (LCUs) are crucial part of dental professionals’ daily practice, in addition to contemporary insight and knowledge [1, 2]. Several studies have reported insufficient knowledge and competence among dental practitioners worldwide [11-13].
In Saudi Arabia, similar studies have assessed dental practitioners at the national level, with some specifically focusing on the Central Region [14-19]. However, due to geographic, demographic, and cultural variations across the country, the available data cannot be generalized. Consequently, there remains a gap in understanding the current level of knowledge and competence among dentists in both the governmental and private sectors in the Western Region. Therefore, this study aims to assess the knowledge and clinical practices related to light-curing units (LCUs) among dental professionals in the Western Region of Saudi Arabia.
2. MATERIALS AND METHODS
A cross-sectional survey was conducted over a duration of three months, among general dentists and specialists of various specialties, working in the governmental and private sectors in the Western Region of Saudi Arabia. Only dental clinicians who use LCUs and work in the Western Region were included in this study. Ethical approval was obtained from the Institutional Review Board of Umm Al-Qura University, Saudi Arabia (registration. No. HAPO-02-K-012).
The questionnaire consisted of thirty-five questions across five sections. The first section was an informed consent. The second section comprised demographic information. The third section assessed knowledge of LCUs and material science. The fourth section focused on clinical practice. The fifth section was related to the maintenance of LCUs. The final section was related to the participants’ satisfaction level in terms of knowledge and clinical practice. All questions were mandatory, which ensured that no missing data were present. Additionally, a pilot study was conducted to validate the questionnaire, ensuring its accuracy and reliability. The questionnaire was administered to the same group of participants with a washout period of two weeks and test-retest was performed. The internal consistency of the survey instrument was assessed using Cronbach’s alpha, which yielded a value of 0.8, indicating good reliability.
The sample size was assessed using a sample size calculator, which estimated a minimum participation of 365 dentist; eventually 500 dental clinicians were invited to the study using the validated questionnaire, hosted by Google Forms, which was distributed electronically via e-mail, social media channels, and personal contacts.
Data analysis was performed using SPSS version 26.0 statistical software (IBM Inc., Chicago, USA). Descriptive statistics and Pearson's chi-squared test for the relevant associations were performed at a significance level of 0.05.
3. RESULTS
A total of 392 responses were collected, achieving a response rate of 78.4%. Respondents who did not use LCUs or were from outside the Western Region of Saudi Arabia were excluded (n=13). The study predominantly involved 249 (65.7%) general dentists, with 268 (70.7%) in the age group ranging from 20 to 29 years, and clinical experience of less than five years for 247 (65.2%). Most respondents (249; 65.7%) reported DDS/BDS as the highest academic degree, followed by PhD (58; 15.3%) and board certification (35; 9.2%). Most academic degrees were obtained from Saudi Arabia (292; 77%), followed by Egypt (29; 7.7%) and the United States (27; 7.1%). Most respondents were working in Jeddah (214; 56.5%), followed by Makkah (121; 31.9%), Taif (28; 7.4%) and Medina (16; 4.2%) (Table 1).
The knowledge of LCUs and material science of participants is presented in Table 2. Most of the participants (277; 73.1%) in the study utilized LCUs and light-activated materials daily. A significant portion of the participants (203; 53.6%) lacked knowledge about the photo-initiator system used in the light-activated materials. Additionally, most participants (238; 62.8%) were unsure if their LCUs emit compatible wavelength with the photo-initiators in the used material. Among all specialties, 22 out of 26 operative specialists (84.6%) reported high knowledge regarding the incorporated photo-initiator systems in light-activated materials and their compatible wavelengths (Fig. 1a). This knowledge level showed a statistically significant difference compared to all other specialties (p < 0.001). Additionally, there was a significant correlation between the highest academic degree earned (p < 0.001), the clinical years of experience (p =0.001) and the level of knowledge about photo-initiator systems and LCU wavelengths. Participants with board certifications, MSc, or PhD degrees demonstrated superior knowledge in these areas (Fig. 1b), as well as those with more than ten years of clinical experience, compared to others within the same category.
A total of 292 (77%) participants acknowledged the link between inadequate radiant exposure and the longevity of the restorations. Most participants agreed that inadequate polymerization leads to low mechanical properties, low color stability, secondary caries and marginal discoloration. However, less than half of the participants agreed that inadequate polymerization leads to more bacterial colonization, toxic reactions, allergic reactions, and tooth sensitivity.
More than half of the participants (206; 54.4%) were unsure about the minimum irradiance of light-curing units required for sufficient polymerization. Regardless of clinical specialty, highest academic degree earned, or years of experience, only 22 participants (5.8%) correctly identified the required irradiance as greater than 500 mW/cm2.
| Variables | - | Total n | Total % |
|---|---|---|---|
| Age | 20-29 | 268 | 70.7 |
| 30-39 | 70 | 18.5 | |
| 40-49 | 28 | 7.4 | |
| More than 50 | 13 | 3.4 | |
| Gender | Male | 165 | 43.5 |
| Female | 214 | 56.5 | |
| Type of practice | Governmental | 301 | 79.4 |
| Private | 43 | 11.3 | |
| Both | 35 | 9.2 | |
| Location of your practice | Makkah | 121 | 31.9 |
| Jeddah | 214 | 56.5 | |
| Medina | 16 | 4.2 | |
| Taif | 28 | 7.4 | |
| Highest earned academic degree | DDS/BDS | 249 | 65.7 |
| Clinical certificate | 15 | 4 | |
| Board certificate | 35 | 9.2 | |
| MSc | 22 | 5.8 | |
| PhD | 58 | 15.3 | |
| Specialty | General Dentistry | 249 | 65.7 |
| Operative Dentistry | 26 | 6.9 | |
| Pediatric Dentistry | 23 | 6.1 | |
| Prosthodontics | 20 | 5.3 | |
| Endodontics | 21 | 5.5 | |
| Orthodontics | 22 | 5.8 | |
| Periodontics | 8 | 2.1 | |
| Dental Public Health | 6 | 1.6 | |
| Others | 4 | 1.1 | |
| Where did you earn your highest degree from? | Saudi Arabia | 292 | 77 |
| Canada | 2 | 0.5 | |
| United States | 27 | 7.1 | |
| United Kingdom | 15 | 4 | |
| Sweden | 5 | 1.3 | |
| Australia | 1 | 0.3 | |
| Japan | 1 | 0.3 | |
| Egypt | 29 | 7.7 | |
| Jordan | 2 | 0.5 | |
| Others | 5 | 1.3 | |
| Clinical experience (in years) | <5 | 247 | 65.2 |
| 5-10 | 75 | 19.8 | |
| >10 | 57 | 15 |
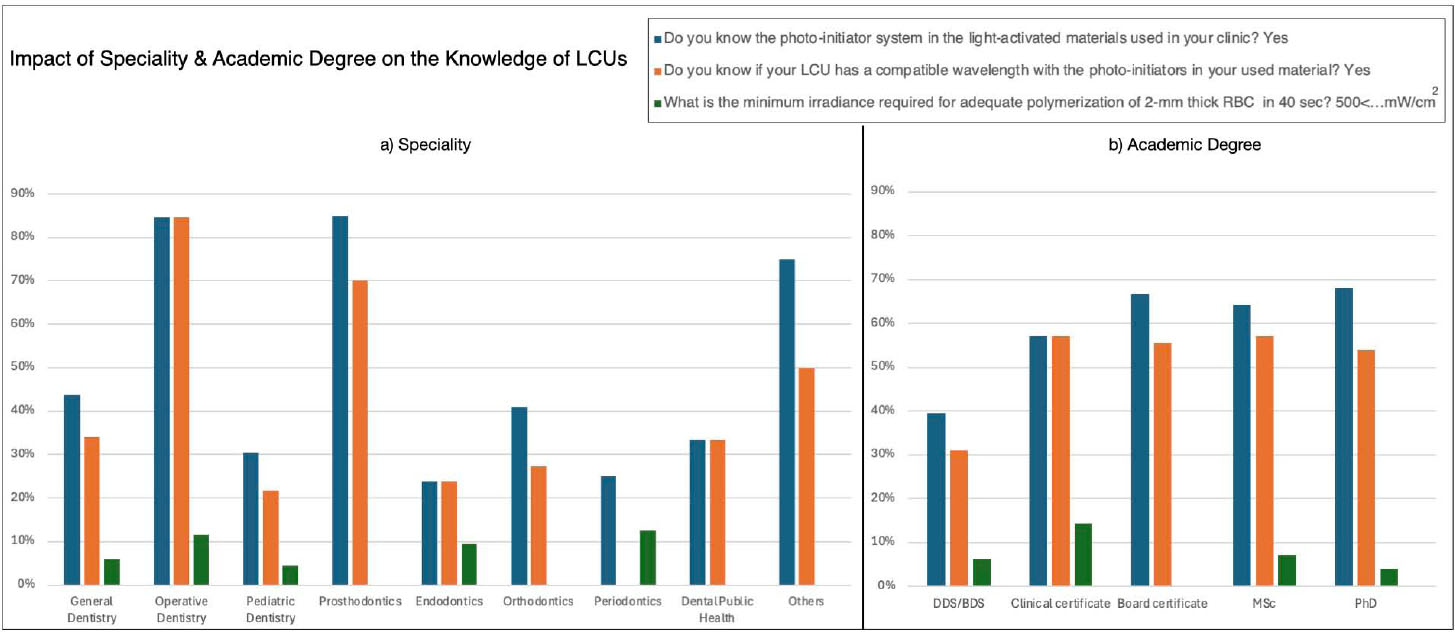
Knowledge of LCUs and materials science among the participants by (a) specialty and (b) academic degree (data reflect percentages of proper knowledge).
| Questions | Response | Total n | Total % |
|---|---|---|---|
| Do you know the photo-initiator system in the light-activated materials used in your clinic? | Yes* | 176 | 46.4 |
| No | 203 | 53.6 | |
| Do you know if your LCU has a compatible wavelength with the photo-initiators in your material? | Yes* | 141 | 37.2 |
| No | 238 | 62.8 | |
| Do you think sufficient radiant exposure is a crucial factor in the longevity of the restoration? | Yes* | 292 | 77 |
| No | 87 | 23 | |
| How often do you use LCU and light-activated materials in your clinical practice? | Daily | 277 | 73.1 |
| Weekly | 76 | 20.1 | |
| Rarely | 24 | 6.3 | |
| Never | 2 | 0.5 | |
| Which of the following can be associated with insufficient radiant exposure (inadequate polymerization)? Please check all that apply. | Low mechanical properties | 308 | 81.3 |
| Low color stability | 264 | 69.7 | |
| More bacterial colonization | 159 | 42 | |
| Toxic reactions | 89 | 23.5 | |
| Allergic reactions | 84 | 22.2 | |
| Secondary caries | 221 | 58.3 | |
| Marginal leakage | 280 | 73.9 | |
| Marginal discoloration | 233 | 61.5 | |
| Tooth sensitivity | 164 | 43.3 | |
| Unsure | 19 | 5 | |
| What's the minimum irradiance required for adequate polymerization of 2-mm thick composites in 40 seconds? | 100-300 mW/cm2 | 22 | 5.8 |
| 300-500 mW/cm2 | 129 | 34 | |
| >500 mW/cm2* | 22 | 5.8 | |
| Unsure | 206 | 54.4 | |
| What is the infection-control technique that has the least negative effect on light-curing tips? | Autoclaving | 56 | 14.8 |
| Disinfectant solution | 83 | 21.9 | |
| Clear barrier* | 161 | 42.5 | |
| Unsure | 79 | 20.8 | |
| What is/are your source/s of information regarding LCUs and light-activated materials? Please check all that apply. | Textbooks | 179 | 47.2 |
| Scientific journals | 143 | 37.7 | |
| Lectures in an undergraduate curriculum | 279 | 73.6 | |
| Lectures in a postgraduate curriculum | 49 | 12.9 | |
| CE lecture including conferences | 41 | 10.8 | |
| Manufactures booklet | 91 | 24 | |
| Internet and social media | 116 | 30.6 |
| Questions | Response | Total n | Total % |
|---|---|---|---|
| What type of LCU are you using? | Quartz-tungsten-halogen lights (QTH) | 24 | 6.3 |
| Plasma-arc lights (PAC) | 1 | 0.3 | |
| Argon-ion lasers | 3 | 0.8 | |
| Light-emitting diodes (LED) | 225 | 59.4 | |
| Unsure | 126 | 33.2 | |
| Which curing mode do you use for curing your restoration? | Soft start | 43 | 11.3 |
| Fast cure | 59 | 15.6 | |
| Conventional mode | 199 | 52.5 | |
| I don’t check the curing mode on my device | 78 | 20.6 | |
| How long do you light-cure a resin-based composite restoration? | 10 seconds for each 2 mm increment | 68 | 17.9 |
| 20 seconds for each 2 mm increment * | 248 | 65.4 | |
| 40 seconds for each 2 mm increment | 55 | 14.5 | |
| 60 second for the bulk restoration | 8 | 2.1 | |
| Location and morphology of the tooth can affect the position between the LCU tip and the resin material surface. The dentist should always aim to: | Hold the light-curing tip as close as possible to the restoration surface * | 262 | 69.1 |
| Hold the light-curing tip up to 10 mm | 22 | 5.8 | |
| Position the light-curing tip at 45-degree angle | 16 | 4.2 | |
| Position the light-curing tip at 90-degree angle | 79 | 20.8 | |
| To increase the overall radiant exposure during curing your restoration, you might need to: | Store RBC material in a refrigerator before clinical application | 127 | 33.5 |
| Increase the curing time more than manufacturer’s recommendation * | 214 | 56.5 | |
| Choose darker shade of RBC | 38 | 10 | |
| What do you mostly use to protect your eyes from “blue light hazards”? | Light shield mounted to LCU | 70 | 18.5 |
| Hand-held light shield | 22 | 5.8 | |
| Orange protective glasses | 112 | 29.6 | |
| My assistant does the curing | 31 | 8.2 | |
| I look away from the blue light | 144 | 38 |
The primary source of information for most participants about LCUs was lectures during their undergraduate curriculum (279; 73.6%), while the lowest source was reported for CE lectures and conferences (41; 10.8%).
The clinical practices related to LCUs among dentists in the Western Region of Saudi Arabia are presented in Table 3. Most participants (225; 59.4%) used LED LCUs. About 199 (52.5%) dentists employed the conventional curing mode for their restorations, while 78 (20.6%) did not check the curing mode before application. Most participants reported the correct curing time and tip position for LCUs. Moreover, 214 (56.5%) of the participants increased the curing time beyond the manufacturer's recommendation to compensate for reduced power output from LCUs.
General dentists, operative specialists, and prosthodontists exhibited significantly superior clinical practices compared to other specialties (p < 0.05) (Fig. 2a). Participants with board certifications demonstrated notably better clinical practice than those with other academic degrees (p < 0.001) (Fig. 2b). Additionally, those with fewer than five years of clinical experience showed significantly better clinical practices (p < 0.05).
Regarding the methods used for eye protection against blue light hazards, around 144 (38%) participants reported looking away without using any protective measures, while 112 (29.6%) participants reported using orange protective glasses.
Table 4 presents the maintenance protocols for light-curing units (LCUs). Many participants, (304; 80.2%), were unaware of the expected shelf life of their LCUs. Most participants (250; 66%) did not control the maintenance of their LCUs or followed the manufacturer's maintenance recommendation.
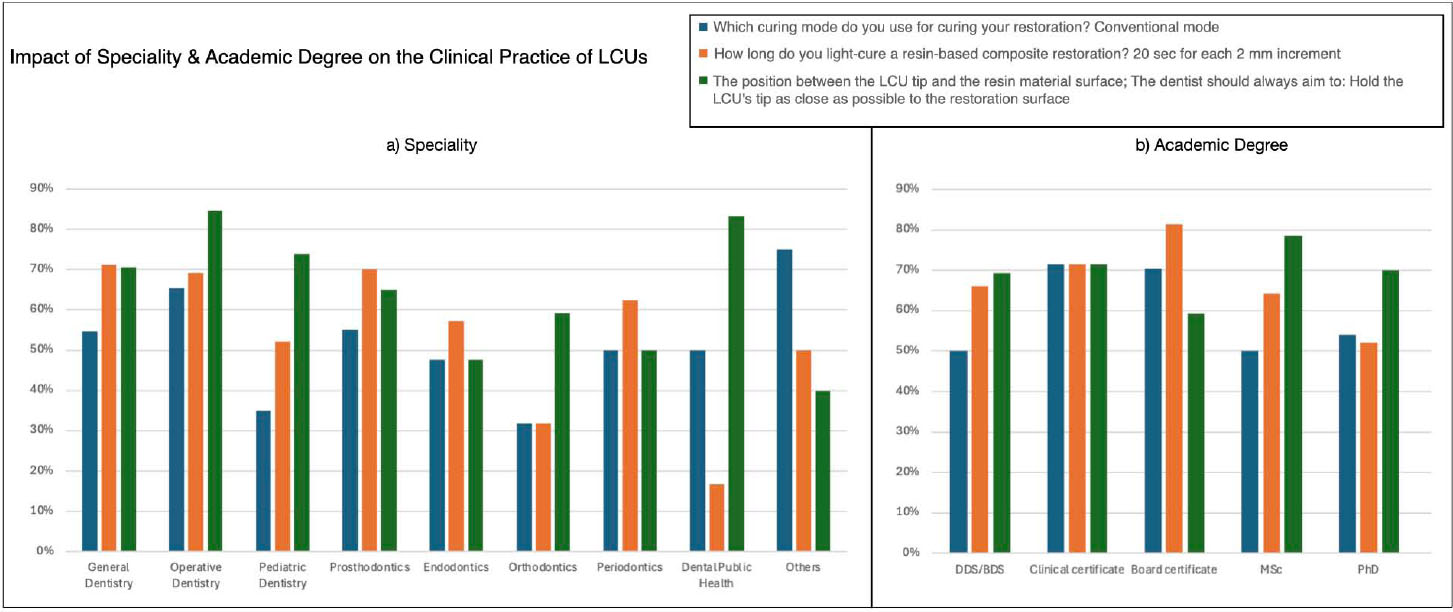
Clinical practice of LCUs among the participants by (a) specialty and (b) academic degree (data reflect percentages of proper practice).
| Questions | Response | Total n | Total % |
|---|---|---|---|
| Do you know the expected shelf life of your light curing unit? | Yes | 75 | 19.8 |
| No | 304 | 80.2 | |
| Do you inspect, clean, and check your LCU before use to ensure it is free of defects and debris and it is on the correct setting? | Yes | 255 | 67.3 |
| No | 124 | 32.7 | |
| Do you control the maintenance of your light curing unit and follow the manufacturer's maintenance recommendation? | Yes | 129 | 34 |
| No | 250 | 66 | |
| How often do you maintain your device? | 1-3 months | 17 | 4.5 |
| 3-6 months | 30 | 7.9 | |
| 6-12 months | 41 | 10.8 | |
| >12 months | 19 | 5 | |
| I don’t maintain my device | 272 | 71.8 | |
| Do you use a dental radiometer to monitor the irradiance of your LCU? | Yes | 48 | 12.7 |
| No | 84 | 22.2 | |
| Not familiar with this device | 247 | 65.2 | |
| How often do you check the irradiance level (output) of your device? | 1-3 months | 19 | 5 |
| 3-6 months | 14 | 3.7 | |
| 6-12 months | 34 | 9 | |
| >12 months | 6 | 1.6 | |
| I don’t maintain my device | 306 | 80.7 |
Most of the participants (255; 67.3%) cleaned their LCUs prior to usage. However, most of the participants (247; 65.2%) were unfamiliar with dental radiometers used to monitor LCU irradiance levels, and 306 (80.7%) did not check the irradiance level (output) of their device.
There was a statistically significant association between the maintenance of light-curing units and the participants’ specialty (p = 0.001), highest academic degree earned (p = 0.015), and clinical experience (p < 0.001). Operative specialists and prosthodontists generally maintained their devices better than other specialties. Participants with board certifications and MSc degrees reported following proper maintenance protocols, as did those with more than ten years of clinical experience.
The levels of satisfaction of the participants were reported in Table 5. Nearly half of the participants expressed moderate to high satisfaction with their knowledge level, clinical practice, training received in dental programs, and available continuing education courses related to the LCU and its clinical practice.
| Questions | Response | Total n | Total % |
|---|---|---|---|
| Are you satisfied with your light curing unit? | Satisfied | 216 | 57 |
| Moderately satisfied | 155 | 40.9 | |
| Dissatisfied | 8 | 2.1 | |
| Are you satisfied with your knowledge level about LCUs and light-activated materials? | Satisfied | 125 | 33 |
| Moderately satisfied | 193 | 50.9 | |
| Dissatisfied | 61 | 16.1 | |
| Are you satisfied with your clinical practice regarding the application of LCU and light-activated materials? | Satisfied | 178 | 47 |
| Moderately satisfied | 178 | 47 | |
| Dissatisfied | 23 | 6.1 | |
| Are you satisfied with the training level in dental programs regarding the clinical practice of LCUs? | Satisfied | 127 | 33.5 |
| Moderately satisfied | 187 | 49.3 | |
| Dissatisfied | 65 | 17.2 | |
| Are you satisfied with the offered continuing education courses related to the LCU and its clinical practice? | Satisfied | 112 | 29.6 |
| Moderately satisfied | 197 | 52 | |
| Dissatisfied | 70 | 18.5 |
Despite the difference in the highest academic degree earned and years of experience, most participants reported high satisfaction with their LCUs and moderate satisfaction with their knowledge and received training. Orthodontists and prosthodontists, followed by operative specialists reported high level of satisfaction. Their responses showed a statistically significant difference compared to other specialists (p = 0.003).
In terms of clinical practice of LCUs, more than half of the specialists reported a high level of satisfaction, except for general dentists (p = 0.003).
4. DISCUSSION
The aim of this study was to assess the attitudes and competence of dental professionals regarding light-curing units (LCUs) in the Western Region of Saudi Arabia, focusing on their knowledge, clinical practice, maintenance of LCUs, and level of satisfaction. Previous investigations conducted in Saudi Arabia have highlighted a significant gap in dentists' knowledge and awareness regarding LCUs. Several studies [17-19] evaluated practitioners' awareness across Saudi Arabia, while others [16, 17] focused specifically on the Central Region. Due to the unique demographic and cultural context of Saudi Arabia, the regional focus of this study is significant, as it provides insights into different sectors within the Western Region, complementing previous studies and addressing a critical gap in the literature. This region Medina includes major cities such as Jeddah, Makkah, and Madinah, which serve as focal points for dental education, training, and practice in Saudi Arabia.
Our findings revealed insufficient knowledge regarding light-activated materials and the appropriate parameters of LCUs. A significant portion of the participants were unaware of the photo-initiator system used in restorative materials. Several studies have emphasized the importance of specific criteria for the emitted light for effective polymerization, including sufficient irradiance and a spectrum emission matching the needs of activating the photo-initiator system [2, 5, 6]. The activation of the photo-initiator in RBCs occurs at a specific wavelength that should align with the absorption spectrum of the material [2, 5, 6]. The lack of understanding of these fundamental concepts coincides with results reported by other researchers [12, 13].
The importance of proper polymerization of RBCs cannot be overstated, as it directly affects the longevity of the restoration and its overall clinical performance [6, 9, 10]. The findings indicate that most participants attributed low mechanical properties to poor polymerization, followed by concerns about marginal leakage and low color stability. Only a few participants recognized the risks of toxic and allergic reactions due to inadequate polymerization. These results align with previous studies reporting a similarly low level of awareness [12, 13, 17]. It is crucial for dental professionals to have a comprehensive understanding of the potential side effects and clinical symptoms associated with improper polymerization of RBCs in order to address these issues effectively.
The polymerization of RBCs is influenced by many factors, including curing mode, curing time, and distance of the light tip from the restoration [1, 4, 7, 8]. This study reported acceptable clinical practices among participants regarding the identification of the LCU used, selection of the appropriate curing mode, application of the proper curing duration, and correct positioning of LCUs. These findings align with other studies [13, 18, 19]. Interestingly, there was an inconsistency between the acceptable clinical practices observed and the insufficient knowledge demonstrated by the participants. This implies that the clinical practice of light curing may be performed out of habit rather than through a comprehensive understanding of the process. This is crucial because the polymerization of light-activated materials is dynamic, and clinical parameters can change based on the situation. Dental professionals should possess sufficient knowledge and competence to handle these situations based on evidence-based knowledge.
The maintenance of LCUs is essential for ensuring their optimal performance and longevity. The curing tip should be kept clean and free of debris and should be regularly checked using a radiometer to confirm that it is delivering adequate intensity for effective polymerization. However, the study revealed a low level of awareness regarding LCU maintenance and its applications, which is consistent with previous studies [14, 16, 18].
Many investigations measuring the irradiance of LCUs have reported that most of LCUs deliver less than 400 mW/cm2, likely due to inadequate maintenance [6, 14, 20, 21]. Our findings revealed that most participants were not familiar with the life expectancy of their LCUs. These findings underscore the need for increased education and training on the proper maintenance of LCUs to ensure their effectiveness in clinical practice.
The current results indicate an insufficient level of knowledge regarding LCUs and light-activated materials. There was a notable association between the level of knowledge and the specialty, with operative specialists and prosthodontists reporting superior expertise. Additionally, dentists with board certification, MSc, and PhD qualifications demonstrated higher knowledge in this area. This disparity could be attributed to the comprehensive education and training these advanced qualifications entail, which likely include more in-depth coverage of LCUs and light-activated materials.
Most participants expressed satisfaction with their LCUs regarding their knowledge level, clinical practice, training, and available continuing education courses. However, this level of satisfaction does not align with the actual knowledge reported by the same group. Many participants learned about LCUs and light-activated materials through undergraduate lectures, followed by textbooks and scientific journals, reflecting their demographic as mostly general dentists with less than five years of clinical experience. This suggests that the undergraduate curriculum should be a focal point for students and course staff, emphasizing the importance of this topic. A similar study conducted in Saudi Arabia highlighted the need to reinforce knowledge regarding LCUs in dental curricula and recommended that dentists enhance their training through continuing education courses [17].
This study sampled the Western Region of Saudi Arabia, with participants from diverse specialties and academic backgrounds, enhancing understanding through varied perspectives. Examining the association between these factors and reported knowledge and practice can help identify the origins of deficiencies and generate more precise recommendations and action plans. Additionally, the study explored aspects beyond knowledge, such as clinical practice and maintenance of LCUs, making it broader compared to previous studies [11, 16, 18].
The study has certain limitations, including unequal responses from different cities, which could introduce geographical bias into the findings. Additionally, the sample predominantly consists of general practitioners with less than five years of experience. The distribution of the majority of general dentists is consistent with the dental workforce data reported in 2022 [22]; however, it may not accurately reflect the demographics of more experienced practitioners or dental specialists. The statistical analysis conducted evaluated the impact of experience level and specialization on LCU-related knowledge and practice, ensuring that potential variations among different practitioner groups were considered and overgeneralization was avoided.
The sample primarily consists of young practitioners, particularly those between 20 and 29 years old, which may limit the generalizability of the findings to more experienced clinicians. This likely reflects a recruitment bias, possibly due to greater accessibility or a higher willingness to participate among younger dentists. National data indicates that the mean age of licensed dentists in Saudi Arabia is approximately 37.7 years [22, 23]. While specific age distribution data for the Western Region is limited, it is reasonable to assume that our findings underrepresent the knowledge and practices of older, more experienced practitioners. This could potentially skew the results toward more recent educational trends or training in the use of light curing units (LCUs), which may not accurately reflect the familiarity with newer technologies or adherence to current guidelines among older practitioners in the region.
CONCLUSION
In conclusion, dental practitioners in the Western Region of Saudi Arabia exhibited inadequate knowledge regarding light-activated restorations and the use of LCUs, as well as improper maintenance, potentially affecting the longevity of restorations. Although participants expressed high satisfaction with their LCU-related knowledge and practices, a clear gap exists between perceived and actual knowledge. The reported clinical practice in the tested area is acceptable but lacks an evidence-based foundation, which is crucial for navigating various clinical situations effectively. As the study included predominantly younger dentists, it reflects the importance of comprehensive educational programs and ongoing training on LCUs which are essential to bridge this gap, ensuring optimal clinical outcomes and more effective use of LCUs.
AUTHORS' CONTRIBUTIONS
The authors confirm their contribution to the paper as follows: R.M.A., A.A.N.: Study conception and design; Z.O..A., R.A.A., M.A., M.A.A.: Data collection; R.M.A., Z.O.A., A.A.N.: Data analysis or interpretation; R.M.A., A.A.N.: Methodology; R.M.A., Z.O.A., R.A.A., A.A.N.: Draft manuscript. All authors reviewed the results and approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| LED | = Light emitting diode |
| LCU | = Light curing unit |
| RBC | = Resin-based composite |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The study was approved by the ethical research committee at Umm Al-Qura University, Faculty of Dentistry, Makkah, Saudi Arabia (IRB no. HAPO-02-K-012)
HUMAN AND ANIMAL RIGHTS
All human research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentations (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2013.
AVAILABILITY OF DATA AND MATERIALS
The data supporting the findings of the article will be available from the corresponding author [R.A] upon reasonable request.
ACKNOWLEDGEMENTS
The authors would like to express our sincere gratitude to the dental practitioners in the Western Region of Saudi Arabia for their invaluable participation and willingness to share their insights.

