All published articles of this journal are available on ScienceDirect.

Early Primary Molar Loss and Associated Factors among Institutionalized Orphans in Yemen
Authors Info & Affiliations
Abstract
Introduction
This study was performed to evaluate the prevalence of early loss of primary molars among institutionalized orphans aged 6–10 years in two Yemeni governorates.
Methods
A cross-sectional survey was conducted on children residing in orphanages in two governorates in Yemen. A total of 644 children (420 males and 224 females) were examined. Data were collected through interviews and clinical examinations using a standardized form, which recorded demographic information, missing primary molars, and other dental conditions. The International Caries Detection and Assessment System II and criteria for factors contributing to tooth extraction were utilized. Occlusal status and arch relations were also assessed. All relevant data were analyzed using SPSS software. A chi-square test was used to determine associations between variables at a significance level of p <0.05.
Results
About 7.8% of the children had early loss of primary molars. The prevalence of different types of malocclusions was not significantly different between the two governorates (p = 0.921). The present study underscores the high incidence of Class II malocclusion at 35.8%, and Molar hypomineralization was recorded at 4.3% with no statistically significant difference between the two governorates (p=0.285). The first molar of the left mandible was the most commonly absent tooth in the dental arch. The 4.7% early molar loss of orphans from Al-Hodeidah was higher than that (3.1%) for molar teeth in Ibb City, and the difference was statistically significant (p = 0.003).
Discussion
The significant regional differences were likely linked to disparities in access to dental care and socioeconomic status. Although caries prevalence was relatively low, it varied by gender and age. These findings underscore the need for early preventive dental care and region-specific oral health interventions.
Conclusion
A high percentage of early loss of primary molar teeth was prevalent, and the mandibular primary molars were the most frequently lost teeth, with regional differences that warrant targeted dental health interventions. These findings highlight the need for early dental care, preventive programs, space maintainers, regional prioritization, and training for caregivers to reduce the long-term oral health impacts on orphans.
1. INTRODUCTION
The United Nations International Children's Emergency Fund (UNICEF) outlines an orphan as a child who has lost one or both parents or been abandoned by them before age eighteen [1, 2]. Most orphans are raised in orphanage institutions, which provide them with housing, shelter, social services, education, and medical care [3]. The socioeconomic standing of the institutionalized orphans, combined with overcapacity, low caretaker-to-child ratio, inadequate nutrition, and the undervaluation of dental care’s importance by caregivers, are causative aspects that compromise the oral health conditions [4, 5]. Orphans, compared to children with parents, show higher rates of dental caries, pain, trauma, and poorer oral hygiene [6-10].
Primary teeth are responsible for chewing, verbal capabilities, and speech, and they stimulate the development of the stomatognathic system, the complex system that includes the jaw, teeth, and associated muscles and tissues involved in chewing and speaking [11]. Premature tooth loss and early exfoliation of anterior and posterior primary teeth are demarcated as losing teeth in the oral cavity earlier than the normal predictable time. Local and systemic factors can be attributed to this phenomenon [12-14]. Premature Loss Of Primary Teeth (PLPT) can affect children’s phonation, producing speech alteration [15, 16]. The preservation of primary jaw integrity strongly influences the progress of permanent successors. Malocclusions—misalignments of teeth when the jaws are closed—are often associated with early tooth loss and may require orthodontic intervention, such as the use of space maintainers to prevent shifting of teeth [15]. Other PLPT includes tooth rotation, crowding of teeth, extrusion of the opposing tooth, craniofacial growth variances, development of deleterious habits, and, precisely, impaction of the erupting permanent tooth and dental jaws measurement discrepancy [15, 17]. Children with PLPT may need orthodontic treatment up to three times more frequently than those without premature loss of primary teeth [15]. Different types of space maintainers are generally used in the upper and lower dental arches of children to aid in preserving arch length following the premature loss of a primary tooth, thereby minimizing the future need for orthodontic intervention [12, 18]. Premature tooth loss negatively impacts children's aesthetic, social, and quality of life [13].
In Yemen, a study on institutionalized orphans in Sana'a found a higher prevalence of traumatized teeth among orphans compared to non-orphans (p < 0.01). Orphans also had a high incidence of oral mucosal lesions and poor oral hygiene, although their dental caries rate was lower (84.7% vs. 89.61% for controls) without significant difference [9]. In Libya, research indicated that higher father education levels correlated with lower dental caries in children, suggesting parental education can improve oral health for orphans as well [19]. Egyptian studies on institutionalized orphans showed high dental caries rates and poor oral health compared to parented children, likely due to inadequate resources [6]. In India, young orphans (5-14 years) in orphanages faced dental trauma and untreated injuries, with caries levels exceeding the WHO target of a mean DMFT/dmft of 1.5, indicating poor dental practices [20]. In other study, orphans also exhibited high dental caries rates, linked to dietary issues, highlighting the impact of environmental factors on their oral health [21]. Another Indian study showed that the caries level in orphans is more than the WHO (Oral Health Goals 2010) target of a mean DMFT/dmft of 1.5. A major difference existed between decayed (dt/DT) and filled (ft/FT) components, indicating poor practices and professional services [22].
Dental health assessment is scarce, particularly that related to primary molar status, and among the orphan population. Therefore, dental health programs should target institutionalized orphans and school children to improve their oral health status and prevent oral diseases. To date, no previous studies have been conducted among orphans in the Ibb and Al-Hodeidah governorates. Moreover, no studies have explored regional variations or molar-specific outcomes. The current study aimed to assess the prevalence, regional differences, and associated risk factors of early primary molar loss among orphans aged 6–10 years in two Yemeni governorates. This study also hypothesizes that there are no regional differences in early primary molar loss among children in two Yemeni governorates.
2. PARTICIPANTS AND METHODOLOGY
2.1. Ethical Consideration
Ethical approval for the study was granted by the University Ibn al-Nafis for Medical Sciences in Yemen (approval number 171, dated 21/12/2023). This study was accomplished in harmony with the ethical values in the Declaration of Helsinki and has fulfilled the guarantees and safeguards for the Faculty of Dentistry Research Ethics Committee.
2.2. Study Design and Setting
A cross-sectional survey was conducted among orphans aged 6–10 years residing in orphanages in two Yemeni cities: Al-Hodeidah (Al-Hodeidah Orphanage) and Ibb (Al-Hobaishi Orphanage and Al-Rahma Orphanage). The recruitment of participants took place over a period of three months, from January 2024 to March 2024. During this time, a meeting was arranged with the primary caregivers. After explaining the aims and objectives of the study, written consent was obtained from their institution's guardian. Children were informed of the study’s benefits and risks and allowed to opt-out if unwilling to participate. All the orphans living in the houses during the study were involved in screening and examination.
2.3. Sample Size Determination
The sample size was determined using G*Power software (http://www.gpower.hhu.de/en.html). It was calculated based on a two-tailed chi-square test. Considering that a moderate effect size (w = 0.4, 4% margin of error) derived from a previous study on primary molar loss, a power of 80%, and a significance level of α = 0.05, the minimum sample size was 600 participants [23]. This was increased to 644 to enhance the precision of the results and ensure a more comprehensive representation of the target population.
2.4. Participants and Eligibility Criteria
Any orphan children aged 6–10 years from both male and female living in an orphanage were included in this study. Data were disaggregated by sex during collection and analysis to explore any potential differences in outcomes. The study followed the Sex and Gender Equity in Research guidelines (SAGER) to ensure appropriate inclusion and reporting of sex-related data [24]. Children whose orphanage administrators refused participation were excluded, also children aged more than 10 years or less than six years. All participants were required to be in good general health, with no history of systemic diseases known to cause tooth agenesis, malformation, or dysplasia.
2.5. Data Collection and Measurement
Data were collected by conducting interviews with selected groups to introduce the procedure that they would be going through. Then, the clinical checkup was carried out independently using a sheet that included details of demographic data and risk factors. The examination team wore full protective equipment, including masks, gloves, and caps. The examination was done using a dental mirror only under a Halogen lamp illuminated light. Before the examination, each tooth was cleaned with gauze and dried with an air syringe.
The screening sheet consisted of two parts. The first part contained the personal information of the orphans, such as gender (male or female), age group (6, 7-8, and 9-10 years, and city (Ibb or AlHodeidah). The second part included the recording of the type of molar missing (1st or 2nd), arch (maxillary or mandibular), and side (right or left). The number of missing primary molars was documented. Furthermore, the presence of space maintainer, stainless crown, and demineralization for primary molars was recorded during data collection and clinical examination.
The International Caries Assessment System II assigns a score ranging from 0 (indicating a sound healthy tooth) to 6 points (indicating an extensive cavity in the dentin) [25, 26] for recording the dentition status of the participant. The evaluation criteria for the factors contributing to tooth extraction based on the classification established by Kay and Blinkhorn (McCaul et al., 2021) were used and recorded as due to caries, either in primary and/or secondary caries, which includes associated complications like periapical abscess and failed pulpotomy [27, 28].
Occlusal status and arch relations of participants from both cities were assessed. The malocclusion measurements were based on the occlusal relations of the first molar in the different age groups according to the criteria described earlier using the standard method. The Classification of Malocclusion was categorized as follows: Class I normal, Class I Malocclusion, Class II Malocclusion, Class III Malocclusion, Mid-line shift, Cross-bite Unilateral, Cross-bite Bilateral, Anterior open bite, Unilateral posterior open bite, Bilateral posterior open bite, Abnormal Overjet, and Abnormal Over-bite and recorded in the form of Yes or No [29, 30].
There were four examiners, two from each city. For calibration, a pilot study was established on 10 orphans from each town, and then the interexaminer reliability test was assessed between the two examiners for Ibb City and the other two examiners in Al-Hodeida, with a substantial agreement result (0.65-0.69, respectively). Furthermore, the intra-examiner reliability test for each examiner’s reading was assessed with substantial to almost perfect agreement results (0.65, 0.70, 0.70, and 0.81)
2.6. Statistical Analysis
All relevant data of orphan participants in both cities were collected and recorded in a custom-designed form. Data were summarized and analyzed as frequencies and percentages by using the Statistical Package for the Social Sciences (SPSS) program (version 26). Associations between variables were determined using Chi-squared tests. A p-value of < 0.05 was considered statistically significant.
3. RESULTS
The study encompassed 644 children aged 6–10 years from two governorates in Yemen, namely, Ibb and Al-Hodeidah. The demographic characteristics of the participants are presented in Table 1. Out of the total participants, 420 were male (65.2%) and 224 were female (34.8%). Gender distribution significantly differed between the two governorates, with Al-Hodeidah having a higher percentage of females (23.9%) than Ibb (10.9%), and Ibb having a higher percentage of males (48.8%) than Al-Hodeidah (16.5%) (p = 0.001). The age distribution showed that the majority of children were in the 9–10 years age group (60.9%), followed by 7–8 years (31.4%) and 6 years (7.8%) (p = 0.001). Fig. (1) shows the prevalence of missing primary molars among Yemeni orphanages. Mandibular first left primary molars (#74) were the most commonly missing teeth (26 primary molars), followed by the mandibular first right primary molars (#84).
As demonstrated in Table 2, the distribution of different dental problems among the two governorates reveals significant disparities. Specifically, 71.4% of children in Al-Hodeidah had at least one carious tooth, in contrast to 38.2% in Ibb, with 17.2% of orphans in Al-Hodeidah having two carious teeth compared to 47.1% in Ibb. Although the presence of three and four-carious teeth was lower overall, these issues were still noted. The two governorates exhibited a significant difference in the total number of carious teeth (p = 0.001). Demineralization was found in 4.3% of the total sample, showing no significant difference between the two governorates (p = 0.285). Furthermore, significant differences emerged in the prevalence of missing primary molars (p = 0.003), with early primary molar loss affecting 7.8% of orphans aged 6–10 years in both Ibb and Al-Hodeidah. Notably, 66.7% of children in Al-Hodeidah had at least one missing molar, while the figure was 60% in Ibb. Three missing primary molars were more prevalent in Al-Hodeidah at 13.3%, with none reported in Ibb, and the percentage of children with four missing primary molars was 6.6% in Al-Hodeidah, absent in Ibb.
| Parameters | Variable | Ibb Governorate N (%) |
Al-Hodeidah Governorate N (%) |
Total N (%) |
|---|---|---|---|---|
| Gender | Male | 314 (48.8%) | 106 (16.5%) | 420 (65.2%) |
| Female | 70 (10.9%) | 154 (23.9%) | 224 (34.8%) | |
| Total | 384 (59.7% | 260 (40.3%) | 644 (100%) | |
| X2 | - | 114.8 | - | |
| p-value | - | 0.001* | - | |
| Age Groups | 6 years | 20 (3.1%) | 30 (4.7%) | 50 (7.8%) |
| 7-8 years | 140 (21.7%) | 62 (9.6%) | 202 (31.3%) | |
| - | 9-10 years | 224 (34.8%) | 168 (26.1%) | 392 (60.9%) |
| Total | 384 (59.6) | 260 (40.4) | 644 (100%) | |
| X2 | - | 16.8 | - | |
| p-value | - | 0.001* | - |
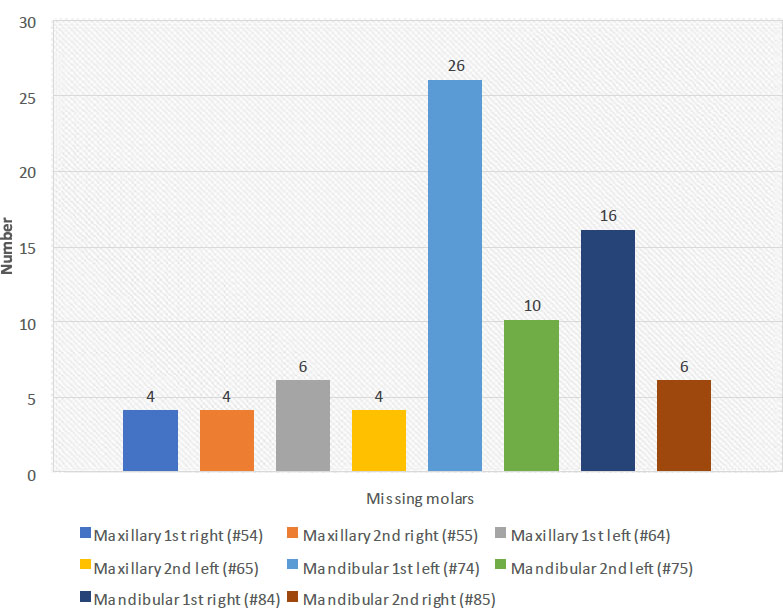
Prevalence of missing molars among Yemeni orphans.
| Parameters | Variable | Ibb Governorate N (%) |
Al-Hodeidah Governorate N (%) |
Total N (%) |
|---|---|---|---|---|
| Number of Carious teeth |
1 carious tooth | 26 (38.2%) | 100 (71.4%) | 126 (60.6%) |
| 2 carious teeth | 32 (47.1%) | 24 (17.2%) | 56 (26.9%) | |
| 3 carious teeth | 10 (14.7%) | 14 (10%) | 24 (11.5%) | |
| 4 carious teeth | 0 (0%) | 2 (1.4%) | 2 (1%) | |
| Total | 68 (100%) | 140 (100%) | 208 (100%) | |
| X2 | - | 25.3 | - | |
| p-value | - | 0.001* | - | |
| Demineralization | Yes | 14 (2.2%) | 14 (2.2%) | 28 (4.3%) |
| No | 370 (57.4%) | 246(38.2%) | 616 (95.7%) | |
| Total | 384 (59.76%) | 260 (40.4%) | 644 (100%) | |
| X2 | - | 1.120 | - | |
| p-value | - | 0.285 | - | |
| Missing Primary molars | 1 missing | 12 (60%) | 20 (66.81%) | 32 (5%) |
| 2 missing | 8 (40%) | 4 (13.3%) | 12 (1.9%) | |
| 3 missing | 0 (0%) | 4 (13,3%) | 4 (0.6%) | |
| 4 missing | 0 (0%) | 2 (6.6%) | 2 (0.3%) | |
| Total | 20(100%) | 30 (100%) | 50 (7.8%) | |
| X2 | - | 16.2 | - | |
| p-value | - | 0.003* | - | |
| Malocclusion | Class II | 18 (33.3%) | 20 (38.5%) | 38 (39.7%) |
| Class III | 2 (3.7%) | 2 (3.8%) | 4 (4.1%) | |
| Anterior Open bite | 4 (7.4%) | 6 (11.5%) | 10 (10.5%) | |
| - | Anterior Cross bite | 2 (3.7%) | 2 (3.8%) | 4 (4.1%) |
| Deep Bite | 12 (29.7%) | 8 (15.5%) | 20 (20.8%) | |
| Posterior Cross bite | 6 (22.2%) | 14 (26.9%) | 20 (20.8%) | |
| Total | 44 (100%) | 52(100%) | 96 (100%) | |
| X2 | - | 1.40 | - | |
| p-value | - | 0.921 | - |
The prevalence of different types of malocclusions was not significantly different between the two governorates (p = 0.921), indicating a similar distribution of malocclusion among children in both regions. Class II malocclusion was the most common type, affecting 35.8% of the children, with slightly higher rates in Al-Hodeidah than in Ibb (38.5% and 33.3%, respectively). Class III had a lower incidence rate (3.8%). Anterior open bite, anterior crossbite, deep bite, and posterior crossbite were also recorded and were slightly evenly distributed between the two governorates (9.4%, 3.8%, 18.9%, and 28.3%, respectively), Table 2.
The distribution of dental caries status for specific teeth was demonstrated in relation to age groups and gender (Table 3). The results showed significant gender differences in caries status for several teeth. For instance, the maxillary first right molar (#54) showed significant gender differences, with males having a higher prevalence of distinct cavities and visual enamel changes than females (p = 0.007). Other teeth, such as the maxillary first left molar (#64) and the mandibular first left molar (#74), showed significant differences in caries distribution between males and females with regard to localized enamel breakdown and underlying dark shadow (p=0.014, and p = 0.021, respectively).
Regarding age groups, the prevalence of caries was significant, with an underlying dark shadow in the maxillary second right molar (#55) in children aged 9–10 years compared with the other age groups (p = 0.001). In the maxillary second left molar (#65), older children showed significant visual changes in enamel and localized enamel breakdown (p = 0.013). Furthermore, a significant difference in the mandibular first right molar (#84, p = 0.048) was detected, with children aged 7– 8 years and 9–10 years having higher recorded visual changes in enamel, localized enamel breakdown, underlying dark shadows, and distinct cavities with visible dentine. Finally, a significant visual change was found in the mandibular second right molar (#85) in older children (p = 0.036), as shown in Table 3.
4. DISCUSSION
Children existing through their families receive physical security, access to food, shelter, and psychological support. However, orphans face less fortunate circumstances and are at a high and complex risk of developing abnormal psychosocial development and are more vulnerable to discrimination and inadequate care due to the absence of parental care [9]. In addition, healthcare in orphanages is often insufficient, leading to untreated health problems, including poor oral health. Limited funding and low caretaker-to-child ratios make it challenging to meet the children's needs adequately [20]. Many studies show a higher incidence of dental issues in orphans [6, 9, 12, 19, 21]. Therefore, the present study was designed to evaluate the prevalence of early primary molar loss and associated risk factors in orphans aged 6–10 years in two Yemeni governorates.
| Tooth | Variable /ICASII | Discolor White or Brown N (%) | Visual Change in Enamel N (%) |
Localized Enamel Breakdown N (%) |
Underlying Dark Shadow N (%) | Distinct Cavity with Visible Dentine N (%) |
|---|---|---|---|---|---|---|
| Gender | ||||||
| #54 | Male | - | 0 | 2 | 2 | 4 |
| Female | 4 | 0 | 0 | 0 | ||
| p-value | - | - | 0.007* | - | - | |
| #55 | Male | - | 2 | 2 | 2 | 2 |
| Female | 2 | 0 | 6 | 0 | ||
| p-value | - | - | 0.113 | - | - | |
| #64 | Male | - | 4 | 10 | 12 | 6 |
| Female | 2 | 0 | 0 | 0 | ||
| p-value | - | - | 0.014* | - | - | |
| #65 | Male | - | 0 | 2 | 2 | 4 |
| Female | 2 | 2 | 0 | 4 | ||
| p-value | - | - | 0.133 | - | - | |
| #74 | Male | - | 2 | 2 | 2 | 10 |
| Female | 0 | 6 | 0 | 2 | ||
| p-value | - | - | 0.021* | - | - | |
| #75 | Male | - | 0 | 6 | 4 | 10 |
| Female | 2 | 2 | 2 | 6 | ||
| p-value | - | - | 0.147 | - | - | |
| #84 | Male | 0 | 4 | 8 | 8 | 4 |
| Female | 2 | 4 | 2 | 4 | 2 | |
| p-value | - | - | 0.253 | - | - | |
| #85 | Male | - | 10 | 8 | - | 6 |
| Female | 6 | 2 | 2 | |||
| p-value | - | - | 0.609 | - | - | |
| Age Groups | ||||||
| #54 | 6 years | - | 2 | 0 | 0 | 0 |
| 7-8 years | 0 | 2 | 0 | 2 | ||
| 9-10 years | 2 | 0 | 2 | 2 | ||
| p-value | - | - | 0.087 | - | - | |
| #55 | 6 years | - | 0 | 2 | 0 | 0 |
| 7-8 years | 2 | 0 | 0 | 0 | ||
| 9-10 years | 2 | 0 | 8 | 2 | ||
| p-value | - | - | 0.001* | - | - | |
| #64 | 6 years | - | 2 | 0 | 0 | 2 |
| 7-8 years | 2 | 0 | 0 | 2 | ||
| 9-10 years | 2 | 6 | 6 | 4 | ||
| p-value | - | - | 0.084 | - | - | |
| #65 | 6 years | - | 2 | 0 | 0 | - |
| 7-8 years | 0 | 4 | 2 | |||
| 9-10 years | 2 | 4 | 2 | |||
| p-value | - | - | 0.013* | - | - | |
| #74 | 6 years | - | - | - | - | - |
| 7-8 years | 0 | 2 | 0 | 2 | ||
| 9-10 years | 2 | 6 | 2 | 10 | ||
| p-value | - | - | 0.755 | - | - | |
| #75 | 6 years | - | - | - | - | - |
| 7-8 years | 0 | 2 | 4 | |||
| 9-10 years | 2 | 6 | 2 | |||
| p-value | - | - | 0.142 | - | - | |
| #84 | 6 years | 0 | 0 | 0 | 2 | 0 |
| 7-8 years | 2 | 2 | 4 | 6 | 6 | |
| 9-10 years | 0 | 6 | 6 | 4 | 0 | |
| p-value | - | - | 0.048* | - | - | |
| #85 | 6 years | - | 0 | 2 | - | 2 |
| 7-8 years | 4 | 6 | 4 | |||
| 9-10 years | 12 | 2 | 2 | |||
| p-value | - | - | 0.036* | - | - | |
The study revealed a 7.8% frequency of early primary molar loss among institutionalized orphans aged 6–10 years in Ibb and Al-Hodeidah. This rate of early molar loss still underscores the significance of oral health challenges faced by these children. A statistically significant difference in the prevalence of early molar loss was found between the two governorates, indicating potential differences in access to dental care and socioeconomic conditions between the two regions. These results contradict previously reported findings since we had a lower prevalence rate than those studies [31-33]. The variation in results could be credited to differences in the target population. Most children in previous studies were non-orphans, and factors such as socioeconomic status, diet, geographic location, and cultural differences may have influenced the outcomes. The lower prevalence in the current study can be attributed to limited access to sticky and sugary snacks in orphanages, a major cause of tooth decay [24, 34].
This study observed that the mandibular left first molar had the highest incidence of missing primary molars (Fig. 1). The same result was found in a study by Murshid et al., who reported that the lower left primary second primary molars were most commonly missing, with the highest rate of premature tooth loss occurring at the age of 8 years [23]. These findings can be correlated to the chronological eruption age of both (first and second) primary molars [35]. The primary first molars, which erupt earlier, tend to remain in the oral cavity longer, increasing their susceptibility to dental caries [36]. Dentists often prioritize the restoration of the second primary molars to maintain space until the first permanent molars erupt [37]. This preference for restoration may explain why the primary 1st molars are more frequently extracted, subsequent by premature loss.
The early extraction of primary molars may significantly impact dental development and occlusion [37]. Such loss can lead to poor chewing habits, including unilateral posterior teeth chewing and anterior teeth chewing [13-15]. Additionally, the loss of these primary teeth can cause the adjacent teeth to shift, which can then affect the occlusal relationship in that area and result in insufficient space for the eruption of permanent teeth [16, 17, 38]. The current study found that class II malocclusion was the most predominant type among the population studied, with no significant difference between government and private facilities. This finding contradicts previous research, such as the study by Mai et al., who reported a higher occurrence of anterior crossbite tendency [39].
Hypomineralization (demineralization) of molars and incisors was first presented in 2001 by Weerheijm et al. and was restricted as “hypomineralization of systemic origin, presenting as demarcated, qualitative defects of the enamel of one to four first permanent molars commonly associated with affected incisors [40].” The present study revealed that 4.3% of the total sample had molar hypomineralisation, a commonly encountered dental condition universal ranging up to 40.2% [41]. Hypomineralized second primary molars among preschool children in Melbourne ranged between 2.7% and 21.8%, which is slightly higher than the value in this study. This outcome can be explained by the fact that they assessed a smaller age group [42].
The incidence of early tooth loss was found in a sample of 50 children, including 26 (52%) males and 24 (48%) females, and the majority of children had one or two teeth prematurely lost (Table 2). These results are consistent with previous findings [30, 31]. The higher incidence of early tooth loss in males may relate to their lower attention to aesthetics and oral hygiene. Caries status also showed significant gender and age differences, with males exhibiting more advanced caries prevalence. Older children (9–10 years) were more likely to have severe caries, underscoring the need for early preventive dental care. This increase in the prevalence of tooth decay might be explained by the delayed admission of some children to the orphanage, which may reflect prior struggles related to certain types of food, hygiene practices, or environmental factors before they enter the care facility. Studies by Al-Maweri and Al-Sufyani reported high caries incidence in Yemeni children with Down syndrome, while Al-Akwa and Al-Maweri found similar trends among primary school children in Yemen [43, 44]. In Saudi Arabia, a study indicated higher caries prevalence among females aged 7–12 [45]. However, in our study, males showed a higher decay percentage, potentially due to the lower number of female participants.
The significant differences in missing primary molars between the two governorates highlight a regional disparity in dental health, possibly due to varying access to dental care and socioeconomic conditions. The consistent prevalence of malocclusion types suggests uniform underlying causes across regions, supporting the need for comprehensive orthodontic care programs that can be uniformly applied in Ibb and Al-Hodeidah. These findings underscore the importance of targeted dental health interventions to address specific regional needs and improve overall dental health outcomes for children in these areas.
A recent systematic review with meta-analysis concluded that institutionalized orphan children are at higher risk of developing dental caries than their parented counterparts. This review went against our findings and could be related to the socioeconomic status in Yemen [46].
Overall, the frequency of early primary molar loss was low among Yemeni orphans (7.8%), and only a few carious teeth were observed. Factors such as rural residence, low self-concept, low salivary barrier capacity, lax food discipline, and frequent consumption of sugary fast food, high plaque index, and infrequent oral hygiene practices (brushing once daily or less) were identified as potential determinants. However, these findings differ from our results, which may be interrelated to the unique socioeconomic status in Yemen, where most of the examined orphaned children were born within the past decade under war conditions and difficult living situations. Consequently, carbohydrate consumption was restricted, leading to decreased caries prevalence as well as a lower incidence of early primary molar loss.
This study has some limitations. It relied on visual examination without using a dental explorer or a radiographic tool, which may have resulted in an increased rate of false-negative diagnoses of dental caries, leading to an underestimation of the true occurrence of caries in the population studied. Additionally, the study was conducted only in three institutions across two Yemeni governorates. Therefore, the findings may not be generalizable to the overall incidence of premature loss of primary teeth amongst children in Yemen. Furthermore, the study did not consider other potential confounders, such as oral hygiene habits and fluoride exposure, on the overall orphan's oral health. Future studies could use a more comprehensive assessment method, such as X-ray-based systems, to address these limitations and investigate risk factors in areas not easily visible during visual examination. Additionally, a larger, more diverse sample size from different regions would be necessary to draw reliable conclusions about the incidence of premature loss of primary teeth amongst children in Yemen.
CONCLUSION
The study highlights a significant prevalence of early primary molar loss among orphaned children in Yemen, with regional differences that warrant targeted dental health interventions.
The findings of this study highlight the urgent need for targeted preventive dental programs in orphanages, focusing on early detection and management of primary molar loss. These programs should include regular dental check-ups and preventive measures, such as the use of preventive orthodontic care or space maintainers, to mitigate the impact of early tooth loss on children's dental development and overall health. Additionally, policymakers should consider implementing school-based dental programs to ensure regular follow-ups and early interventions.
AUTHORS’ CONTRIBUTIONS
The authors confirm their contribution to the paper as follows: T.A.A.D., A.M.S.Q.: Study conception and design; K.K.A., R.M.F.I., M.M.A.M.: Data collection; A.M.A.H.: Data Analysis or Interpretation; A.M.A.M.: Methodology; N.S.: Visualization; T.A.B.: Draft manuscript; B.M.A.M.: Validation. All of the authors have reviewed the results and approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| UNICEF | = United Nations International Children's Emergency Fund |
| PLPT | = Premature Loss of Primary Teeth |
| SAGER | = Sex and Gender Equity in Research guidelines |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Ethical approval for the study was granted by the University Ibn al-Nafis for Medical Sciences in Yemen (approval number 171, dated 21/12/2023). This study fulfilled the guarantees and safeguards for the Faculty of Dentistry Research Ethics Committee.
HUMAN AND ANIMAL RIGHTS
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or research committee and with the 1975 Declaration of Helsinki, as revised in 2013.
CONSENT FOR PUBLICATION
A written consent was obtained from the institution's guardian of the participants.
AVAILABILITY OF DATA AND MATERIALS
The data that support the findings of this study are available from the corresponding author upon reasonable request.
ACKNOWLEDGEMENTS
Declared none.

