All published articles of this journal are available on ScienceDirect.

Perception of Direct-to-Consumer Orthodontics in Saudi Arabia
Authors Info & Affiliations
Abstract
Introduction
Direct-to-consumer orthodontics (DTCO) provides a convenient and affordable alternative to traditional care, utilizing clear aligners. However, its increasing use raises concerns about professional supervision. This study, addressing the limited public perception in Saudi Arabia, assessed interest in and preferences for DTCO versus conventional treatment.
Methods
A descriptive cross-sectional study surveyed 507 Saudi Arabian adults aged 20–60 years. A self-administered questionnaire assessed awareness of DTCO, perceptions, and preferences compared with traditional care. Participants were recruited using convenience sampling via social media and direct outreach. Data were analyzed using SPSS version 20 and chi-squared tests.
Results
While 44% were aware of clear aligners, only 16% recognized DTCO. Nevertheless, 70% would consider DTCO for themselves or their children, primarily due to convenience. Concerns included lack of professional supervision and treatment quality. Notably, 82% considered radiographs essential, and 84% were aware of the risks of unsupervised treatment.
Discussion
Rising interest in DTCO, despite limited awareness of associated risks, suggests that marketing may outweigh clinical understanding, highlighting the need for patient education. Although flexible, DTCO’s lack of professional oversight remains a significant public concern.
Conclusion
Public awareness of DTCO is limited, yet interest is high due to perceived convenience and affordability. However, significant concerns persist regarding supervision, safety, and diagnostic accuracy. These findings underscore the critical need for public education on professionally supervised orthodontic care and the potential complications of unsupervised treatment.
1. INTRODUCTION
Do-it-yourself dentistry and orthodontics have become increasingly popular in recent years, with patients undertaking certain dental procedures without the assistance of dentists or other professionals [1, 2]. Reports have emerged of unlicensed vendors and unauthorized shops selling dental products, such as aligners and whitening kits, without proper regulatory approval, raising significant health and safety concerns. This phenomenon, often referred to as dental quackery, is gaining prevalence worldwide and poses risks of irreversible harm to patients if not properly addressed [3].
As the demand for orthodontic treatment has increased, there is growing curiosity about appliances that are both aesthetically appealing and more convenient than traditional fixed devices [4].
There are many variations of clear aligners, but all share common features: they are removable, transparent, and thermoformed appliances [5]. Variations may occur in terms of the materials used, design, and manufacturing methods. Clear aligners offer several advantages over conventional fixed appliances, including improved oral hygiene and enhanced comfort [6].
Consequently, the use of direct-to-consumer orthodontic (DTCO) appliances has increased rapidly [7]. The concept behind DTCO is to provide orthodontic care in a more affordable and convenient manner. Several companies in the United States actively market these appliances [8]. Customers are typically asked to take dental impressions at home or undergo an intraoral scan at a company location. After a remote evaluation of the digital models by technicians and/or dentists, clear aligners are produced and shipped to the customer along with instructions. Patients then use the appliances to align their teeth without visiting a dental office or receiving close supervision from an orthodontist [9]. Orthodontic organizations and dental boards have expressed concerns about DTCO products being used in place of care from qualified orthodontists [10]. Moreover, the American Dental Association (ADA) opposes DTCO due to the risk of irreversible harm to patients [11].
Since 1997, direct-to-consumer (DTC) services have been utilized in healthcare advertising [12]. The widespread use of DTC drugs and medical devices, combined with effective marketing campaigns and the aesthetic appeal and convenience of clear aligners, may encourage consumers to choose DTCO appliances over visiting an orthodontist. According to Wexler et al. (2020), many consumers opted for DTCO despite professional recommendations for in-office treatment, primarily due to persuasive advertising and perceived convenience [8]. Few studies have evaluated population perceptions and understanding of the advantages and disadvantages of DTCO compared to traditional in-office orthodontic care. Research on this topic remains limited in the United States, and, to our knowledge, no studies have assessed consumer perceptions and preferences in Saudi Arabia or other Arab countries. Therefore, this study aims to examine patients' perceptions of orthodontic treatment and their interest in using DTCO compared to in-office treatment in Saudi Arabia, employing a prefabricated population-based survey.
2. METHODOLOGY
2.1. Study Design
This study employed a descriptive cross-sectional design and was conducted in Saudi Arabia from May 2023 to October 2023.
2.2. Sample Size
The target population comprised 507 adults aged 20–60 years. The sample size was calculated using RaoSoft's online sample size calculator, with a 5% margin of error and a 95% confidence level. This calculation was based on data from the Saudi Central Department of Statistics and Information, considering the total adult population within the specified age range in Saudi Arabia, which is approximately 21.3 million [13].
2.3. Inclusion and Exclusion Criteria
2.3.1. Inclusion Criteria
- Adults aged 20 to 60 years.
- Residents of Saudi Arabia, including both Saudi nationals and non-Saudi residents.
- Both males and females were eligible.
- Individuals who consented to participate by completing the survey.
- Participants with or without prior orthodontic treatment experience.
2.4. Ethical Considerations & Confidentiality
Ethical approval for the study was obtained from the College of Dentistry at Al-Qura University (Approval No. HAPO-02-K-012-2023-04-1579). Prior to participation, all participants were provided with information on the study’s nature and objectives. Informed consent was obtained electronically, with participants confirming their agreement by clicking “Next” before proceeding with the questionnaire. Recruitment took place between May 25, 2023, and October 27, 2023.
2.5. Data Collection Tool (instrument)
Data were collected using a self-administered questionnaire adapted from a previously validated survey [14], consisting solely of closed-ended questions. The questionnaire was translated into Arabic, and back-translation into English was performed by an independent expert to ensure accuracy and consistency with the original version. The questionnaire consisted of two sections: the first section collected demographic and basic information, while the second section included 30 questions assessing participants’ perceptions of direct-to-consumer orthodontics (DTCO), orthodontists, and factors influencing decisions to pursue orthodontic treatment.
2.6. Data Collection and Management
Data were collected between May 25, 2023, and October 27, 2023, using a structured, self-administered online questionnaire. Participants were recruited through digital channels, including social media platforms such as WhatsApp, Instagram, X (formerly Twitter), Snapchat, and Telegram, targeting adults from various regions across Saudi Arabia. No personally identifiable information was collected; each participant was assigned a unique study code and initials to ensure anonymity. Data entry was independently performed by two individuals to maintain accuracy, and after verification, the dataset was securely uploaded to a statistical database for analysis.
2.7. Statistical Analysis Plan
Data were tabulated and analyzed using the Statistical Package for Social Sciences (SPSS v.20). Quantitative variables, such as age, number of children, and education level, were categorized into discrete groups to facilitate descriptive analysis and cross-tabulation. For example, age was grouped into five brackets (16–25, 26–35, etc.), and education levels were classified according to the highest degree obtained. Where applicable, variables were dichotomized (e.g., “familiar with DTCO: yes/no”) to enable chi-square testing. Statistical significance was set at p < 0.05. Categorical data were analyzed using the chi-squared test, and mean ± standard deviation (SD) and proportions were used to summarize the results.
2.8. Potential Sources of Bias
Several potential sources of bias were considered in this study. Selection bias may have arisen from the use of convenience sampling and reliance on social media recruitment, which could favor younger, more tech-savvy participants. To mitigate this, recruitment targeted multiple platforms and regions across Saudi Arabia. Information bias is also possible due to the self-reported nature of the questionnaire. To reduce response bias, the survey was conducted anonymously, and neutral language was used throughout. Additionally, no incentives were provided, minimizing the risk of coercion.
3. RESULTS
A total of 507 participants were included in this study. The demographic characteristics are summarized in Table 1. Sixty-one percent of participants were male, while the remaining 39% were female. Additionally, 80% held a bachelor’s degree or higher, whereas the remaining 20% had a diploma or a high school education. Approximately two-thirds of participants reported considering orthodontic treatment, and 38% believed they had moderate-to-severe malocclusion. Most participants (78%) did not have dental insurance that covered orthodontic treatments.
| Variable | Value | n | % |
|---|---|---|---|
| Please indicate your age group. | 16-25 | 198 | 39.05% |
| 26-35 | 103 | 20.32% | |
| 36-45 | 94 | 18.54% | |
| 46-55 | 63 | 12.43% | |
| more than 55 | 49 | 9.66% | |
| Please indicate your gender. | Male | 310 | 61.14% |
| Female | 197 | 38.86% | |
| Please indicate your region. | Western | 386 | 76.13% |
| Central | 54 | 10.65% | |
| Eastern | 22 | 4.34% | |
| Southern | 27 | 5.33% | |
| Northen | 18 | 3.55% | |
| Please indicate the highest educational level you have completed. | Diploma | 42 | 8.28% |
| High school | 104 | 20.51% | |
| Bachelor | 288 | 56.80% | |
| Master | 46 | 9.07% | |
| MD or DDS/DMD | 5 | 0.99% | |
| PhD | 22 | 4.34% | |
| How many children do you have? | 0 | 240 | 47.34% |
| 1 | 40 | 7.89% | |
| 2 | 76 | 14.99% | |
| 3 | 50 | 9.86% | |
| 4 or more | 101 | 19.92% | |
| Has anybody in your family ever sought orthodontic treatment? | Yes, with regular braces | 291 | 57.40% |
| Yes, with clear (invisible) aligners | 47 | 9.27% | |
| No | 169 | 33.33% | |
| Have you lately thought of getting your teeth straightened or receiving orthodontic treatment? | Seriously considered | 133 | 26.23% |
| Somewhat considered | 104 | 20.51% | |
| Considered, but not seriously | 102 | 20.12% | |
| Did not consider | 168 | 33.14% | |
| If you answered yes to question number 7, How severe do you think your dental malocclusion is, | Severe | 38 | 7.50% |
| Moderate | 154 | 30.37% | |
| Mild | 148 | 29.19% | |
| I do not know | 167 | 32.94% | |
| Do you have dental insurance and provide coverage for orthodontic procedures? | Yes | 57 | 11.24% |
| No | 394 | 77.71% | |
| I don't know | 56 | 11.05% |
Table 2 shows that 44% of the participants reported being familiar with clear aligners, while only 16% were familiar with the DTCO. However, most participants stated they would consider having DTCO (70%) for themselves or their children. Around 54% believed that at-home orthodontic treatment must be supervised by an orthodontist.
| Variable | Value | n | % |
|---|---|---|---|
| Are you familiar with clear (invisible) aligner orthodontics? | Yes | 226 | 44.58% |
| No | 281 | 55.42% | |
| Do you have knowledge of or experience with direct-to-consumer orthodontic treatments or at-home teeth alignment services? | Yes | 79 | 15.58% |
| No | 428 | 84.42% | |
| Are you aware of any acquaintances or relatives who have undergone orthodontic treatment through direct-to-consumer orthodontic services or at-home teeth alignment programs? | Yes | 78 | 15.38% |
| No | 429 | 84.62% | |
| When considering orthodontic intervention, how likely would you be to choose at-home teeth alignment services over visiting an orthodontist's clinical setting? | Extremely likely | 113 | 22.29% |
| Somewhat likely | 139 | 27.42% | |
| Only if I have mild malocclusion | 107 | 21.10% | |
| Extremely unlikely | 148 | 29.19% | |
| Considering a child's perceived need for orthodontic intervention, how inclined would the parent be to pursue direct-to-consumer orthodontic solutions rather than seeking care from a licensed orthodontist's practice? | Extremely likely | 115 | 22.68% |
| Somewhat likely | 140 | 27.61% | |
| Only if I have mild malocclusion | 111 | 21.89% | |
| Extremely unlikely | 141 | 27.81% | |
| What do you think are the primary advantages of receiving orthodontic treatment through at-home teeth alignment services? | Cost | 102 | 20.12% |
| Treatment duration | 32 | 6.31% | |
| Convenience | 212 | 41.81% | |
| Quality of treatment/level of care | 38 | 7.50% | |
| Maintaining adequate oversight of my medical care and preventing damage to my dentition | 34 | 6.71% | |
| Customer service | 44 | 8.68% | |
| Others | 45 | 8.88% | |
| What are your primary concerns with using at-home teeth straightening services for orthodontic treatment? | Cost | 119 | 23.47% |
| Treatment duration | 39 | 7.69% | |
| Convenience | 26 | 5.13% | |
| Quality of treatment/level of care | 103 | 20.32% | |
| Maintaining adequate oversight of my medical care and preventing damage to my dentition | 142 | 28.01% | |
| Customer service | 23 | 4.54% | |
| Others | 55 | 10.85% | |
| Do you believe that obtaining orthodontic treatment through remote teeth alignment services would align your teeth more quickly than conventional braces? | Yes | 170 | 33.53% |
| No | 337 | 66.47% | |
| I don't know | 0 | 0.00% | |
| Do you believe that at-home teeth straightening services provide the same level of dental and orthodontic care as in-person treatment by a dentist or orthodontist in a clinical setting? | Yes | 175 | 34.52% |
| No | 332 | 65.48% | |
| Does orthodontic treatment using at-home teeth straightening services facilitate routine assessments and modifications to the treatment plan as necessary during the course of therapy? | Yes | 255 | 50.30% |
| No | 252 | 49.70% | |
| According to research, do you believe that orthodontic treatment facilitated by at-home teeth straightening services is overseen by an orthodontist? | Yes | 273 | 53.85% |
| No | 234 | 46.15% | |
| Do at-home teeth straightening services effectively treat severe orthodontic issues like overbite, underbite, and crossbite? | Yes | 237 | 46.75% |
| No | 270 | 53.25% |
| Variable | Value | n | % |
|---|---|---|---|
| Do you think that a patient's overbite, underbite, crossbite, or other “extreme” malocclusions can be fixed with orthodontic treatment and at-home teeth straightening services? | Yes | 366 | 72.19% |
| No | 141 | 27.81% | |
| What do you think is the biggest benefit of seeking orthodontic treatment at an orthodontist's office? | Cost | 42 | 8.28% |
| Duration of treatment | 46 | 9.07% | |
| Convenience | 58 | 11.44% | |
| Quality of treatment/level of care | 138 | 27.22% | |
| Ensuring adequate supervision of my treatment and preventing harm to my teeth | 186 | 36.69% | |
| Customer support | 16 | 3.16% | |
| Others factors | 21 | 4.14% | |
| What may be your biggest concern with seeking orthodontic treatment at an orthodontist's office? | Cost | 234 | 46.15% |
| Treatment duration | 90 | 17.75% | |
| Convenience | 31 | 6.11% | |
| Quality of treatment/level of care | 38 | 7.50% | |
| Ensuring optimum supervision of my treatment and avoiding harm to my teeth | 38 | 7.50% | |
| Customer service | 23 | 4.54% | |
| Others | 53 | 10.45% | |
| The majority of orthodontists provide various payment options to meet the needs of their patients. Did you know that? | Yes | 335 | 66.07% |
| No | 172 | 33.93% | |
| Did you know that in addition to traditional braces, many orthodontists also provide clear aligner orthodontics? | Yes | 324 | 63.91% |
| No | 183 | 36.09% | |
| Do you anticipate that radiographic X-rays will be obtained by an orthodontist's office for the purposes of orthodontic diagnosis and treatment planning? | Yes | 407 | 80.28% |
| No | 100 | 19.72% |
Table 3 contains questions regarding patients’ perceptions of treatment in the dental office with a trained orthodontist. Most participants were aware that their orthodontists had pursued specialized orthodontic training programs. However, cost was the biggest concern when considering office treatments (46%).
Table 4 contains questions regarding orthodontic treatment. The participants perceived the benefits of orthodontic treatment as follows: straightening the teeth (75%), improving the smile (70%), improving the bite and functionality of the teeth (66%), and obtaining better facial aesthetics (57%).
| Variable | Value | n | % |
|---|---|---|---|
| What advantages do you believe orthodontic treatment offers? (check all that apply)? | |||
| Straighten teeth | Yes | 381 | 75.15% |
| No | 126 | 24.85% | |
| Improve the bite and function of the teeth | Yes | 337 | 66.47% |
| No | 170 | 33.53% | |
| Eliminating harm to the teeth | Yes | 210 | 41.42% |
| No | 297 | 58.58% | |
| Improve the smile | Yes | 358 | 70.61% |
| No | 149 | 29.39% | |
| Better facial esthetics | Yes | 292 | 57.59% |
| No | 215 | 42.41% | |
| Achieving a stable result | Yes | 222 | 43.79% |
| No | 285 | 56.21% | |
| Do you think that unsupervised tooth movement can result in negative consequences like gum recession? | Yes | 428 | 84.42% |
| No | 79 | 15.58% | |
| Do you believe that adjustments to orthodontic treatment may be required to prevent side effects and guarantee the best possible outcomes? | Yes | 427 | 84.22% |
| No | 80 | 15.78% | |
| Do you believe that radiographic X-rays are an essential component for orthodontic diagnosis and treatment planning? | Yes | 418 | 82.45% |
| No | 89 | 17.55% | |
| How significant would each of the following be in choosing your treatment provider, supposing you are thinking about getting orthodontic treatment for yourself? | |||
| Personal: Cost | Extremely important | 362 | 71.40% |
| Somewhat important | 128 | 25.25% | |
| Not important | 17 | 3.35% | |
| Personal: Convivence | Extremely important | 289 | 57.00% |
| Somewhat important | 181 | 35.70% | |
| Not important | 37 | 7.30% | |
| Personal: Treatment duration | Extremely important | 282 | 55.62% |
| Somewhat important | 186 | 36.69% | |
| Not important | 39 | 7.69% | |
| Personal: Having direct supervision over treatment by an orthodontics | Extremely important | 401 | 79.09% |
| Somewhat important | 85 | 16.77% | |
| Not important | 21 | 4.14% | |
| Personal: Quality of treatment/ level of care | Extremely important | 422 | 83.23% |
| Somewhat important | 69 | 13.61% | |
| Not important | 16 | 3.16% | |
| How significant would each of the following variables be in choosing your kid's treatment provider, supposing you have a child for whom you are contemplating orthodontic treatment? | |||
| Children: Cost | Extremely important | 347 | 68.44% |
| Somewhat important | 129 | 25.44% | |
| Not important | 31 | 6.11% | |
| Children: Convivence | Extremely important | 361 | 71.20% |
| Somewhat important | 125 | 24.65% | |
| Not important | 21 | 4.14% | |
| Children: Treatment duration | Extremely important | 322 | 63.51% |
| Somewhat important | 148 | 29.19% | |
| Not important | 37 | 7.30% | |
| Children: Having direct supervision over treatment by an orthodontics | Extremely important | 423 | 83.43% |
| Somewhat important | 71 | 14.00% | |
| Not important | 13 | 2.56% | |
| Children: Quality of treatment/ level of care | Extremely important | 421 | 83.04% |
| Somewhat important | 66 | 13.02% | |
| Not important | 20 | 3.94% | |
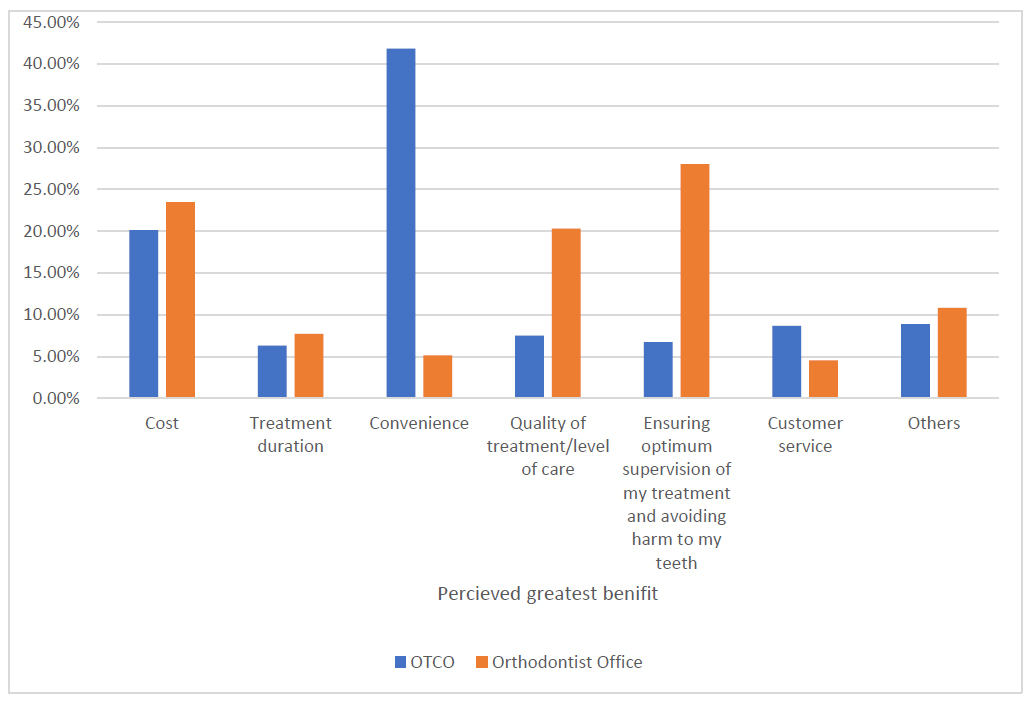
Comparing the DTCO treatment experience with an orthodontist’s office in terms of reported benefits.
Fig. (1) illustrates the factors that participants considered most important when choosing an orthodontic treatment provider. The quality of treatment was rated as the most important factor (83%), followed by direct supervision by an orthodontist (79%). These factors were similarly prioritized when participants responded regarding treatment for their children. Using the Fisher-Freeman-Halton Exact Test (Fig. 1), a significant association was found between participants’ perceived greatest concerns regarding DTCO versus orthodontic office treatment (p < 0.001).
4. DISCUSSION
This study investigated patients’ perceptions and preferences regarding orthodontic treatment options, including traditional in-office treatment and DTCO, within the Saudi population—a topic that remains underrepresented in the literature. A recent study by Felemban OM et al. (2022) [15] examined factors influencing orthodontic decision-making in Saudi Arabia and identified cost, treatment duration, access to qualified providers, confidence in the provider’s ability to manage complications, and appointment availability as key barriers to seeking orthodontic care for both functional and aesthetic concerns. In contrast, factors such as treatment commitment and insurance coverage were perceived as less influential. Our findings provide additional insights and expand upon previous research, highlighting both the growing interest in orthodontic care and the need for enhanced patient education.
The predominance of participants (39%) in the 16–25 age group may be attributed to several factors. This age group represents a highly digitally engaged population, which aligns with the online nature of the survey distribution. They are also the primary users of social media platforms, where awareness of DTCO is commonly promoted through targeted advertising. This observation is supported by Wexler et al. (2020), who found that digital marketing and online visibility significantly influenced younger adults’ interest in and engagement with DTCO services [8].
In this study, 84% of participants demonstrated high awareness of the importance of undergoing orthodontic treatment under professional supervision to avoid adverse treatment effects. This finding aligns with a study conducted in a similar Saudi population, which concluded that the public is highly aware of the quality of orthodontic care provided by licensed orthodontists [16].
The results also showed that 60% of participants considered orthodontic treatment primarily for correcting slight to moderate malocclusion. This is broadly consistent with previous studies conducted in Saudi Arabia, where between 21% and 55.4% of children and adolescents were reported to exhibit signs of malocclusion [17-20].
Awareness of direct-to-consumer orthodontics (DTCO) in our study was substantially lower than that reported in a previous study conducted in the United States, with only 16% of respondents indicating familiarity with DTCO compared to 45% in the U.S. sample [21]. This disparity may be partly attributed to the presence of DTCO companies in the U.S. that actively advertise and promote their services directly to the public. These findings suggest that regional market dynamics and exposure to targeted advertising may significantly influence public awareness.
Our participants indicated that the greatest perceived advantage of pursuing orthodontic care through a remote or at-home treatment approach was convenience (42%), which aligns with a similar study reporting convenience as a major factor influencing patient choice [14]. However, concerns regarding treatment supervision (33%) and potential harm to the teeth (33%) were also prominent among participants. Previous studies have similarly highlighted the risks of unsupervised at-home orthodontic treatments, emphasizing safety and potential physical harm [22]. Notably, Wexler et al. (2020) found that many individuals initially sought consultations with dentists or orthodontists before acquiring direct-to-consumer clear aligners but ultimately chose the DTCO option despite professional recommendations for in-office treatment [8]. This choice is likely influenced by factors such as convenience, cost, and the desire for greater autonomy in managing their orthodontic care.
A recent study involving 1,441 participants examined patients’ perspectives and interest in DTCO compared to seeking care from orthodontists [14]. Convenience was identified by most participants as the primary advantage of using DTCO products, followed by cost. In contrast, the main advantage of visiting an orthodontist was the level of professional care. These findings are consistent with a study by Olson (2020), which surveyed 249 respondents and reported that Americans showed a strong preference for DTCO due to its convenience and affordability [21].
Wexler et al. (2020) [8] conducted the first study evaluating the user experience of at-home teeth aligners using an online survey with 470 respondents. The study found that the vast majority of participants reported either great or average satisfaction with the aligners. Notably, participants who used aligners to correct biting problems were more likely to be dissatisfied compared to those who used them to address crowding or spacing issues.
Participants predominantly recognized orthodontists’ specialized training (Table 3), reflecting the American Association of Orthodontists’ emphasis on qualified professionals overseeing treatment to ensure optimal outcomes [23]. In-office treatment was primarily associated with quality care and complication avoidance (37%), highlighting patients’ prioritization of safety and effectiveness, as supported by previous research [24]. Economically, direct-to-consumer aligners may appeal to cost-conscious individuals; however, patients need to be educated about potential pitfalls and hidden costs [25]. Cost emerged as the main deterrent for in-office treatment (46%), which is unsurprising given that only 22% of participants reported having dental insurance. This aligns with a study conducted in Canada, which found that dental insurance is associated with improved dental attendance and oral health outcomes [26]. These findings underscore the need for orthodontists to consider flexible payment options, such as spreading treatment costs over manageable monthly installments, offering lower fees for upfront payments, providing discounts for multiple family members, and partnering with financing companies to provide extended payment plans with low interest rates, thereby addressing patient preferences and affordability concerns [8].
Participants primarily associated orthodontic treatment with improved aesthetics (straightening teeth, enhancing smile) and functionality (achieving a better bite). However, only a small proportion recognized the importance of attaining stable, long-term results and minimizing potential harm to the teeth. This highlights the need for patient education on the long-term benefits of proper orthodontic care, as emphasized by the American Association of Orthodontists (AAO) [23]. Notably, a high proportion of participants (84%) acknowledged the potential side effects of unsupervised treatment, reflecting an implicit appreciation for the importance of professional supervision. Similarly, the strong emphasis on radiographic assessment (82%) aligns with established diagnostic standards in orthodontics [23].
Although the majority of participants were from the western region of Saudi Arabia, the inclusion of individuals from other regions provides a degree of national representation. However, the overrepresentation of the western region may limit the generalizability of the findings. Future studies should aim for more balanced regional sampling to better capture diverse perspectives. Nevertheless, the observed trends in awareness and attitudes toward DTCO likely reflect patterns among technologically engaged and urban populations, both within Saudi Arabia and potentially in other Gulf countries with similar healthcare access and consumer behaviors.
The quality of treatment and direct supervision by an orthodontist were the most critical factors influencing participants’ choices for themselves and their children. Multiple studies examining factors affecting satisfaction with orthodontic treatment among adults have found that effective communication is essential, and the quality of the doctor-patient relationship is strongly linked to overall treatment satisfaction.
5. LIMITATIONS AND FUTURE RESEARCH
The limitations of this study include potential selection bias due to the recruitment method and reliance on self-reported data. Although the sample included participants from across Saudi Arabia, there was a notable overrepresentation from the western region, which may limit the generalizability of the findings. Additionally, unmeasured confounding variables, such as participants’ socioeconomic status, health literacy, prior dental or orthodontic experience, and exposure to social media marketing, may have influenced perceptions of direct-to-consumer orthodontics. Finally, evaluating the cost-effectiveness of different orthodontic treatment options could provide further insights for both patients and providers [27, 28].
CONCLUSION
This study aimed to explore public awareness, interest, and preferences regarding direct-to-consumer orthodontics (DTCO) versus traditional orthodontic care in Saudi Arabia. The findings revealed that, although awareness of DTCO remains relatively low, a significant proportion of participants expressed interest in using such services, primarily due to perceived convenience and affordability. Nevertheless, concerns regarding treatment supervision, safety, and diagnostic quality were prominent, highlighting a gap between consumer interest and understanding of potential risks.
These results emphasize the critical need for public education to ensure that patients make informed decisions. Dental professionals and regulatory authorities should actively promote awareness of the importance of supervised treatment and the potential risks associated with unsupervised orthodontic care. Overall, the study underscores the necessity of balancing innovation and accessibility with patient safety and clinical oversight.
AUTHORS’ CONTRIBUTIONS
The authors confirm their contributions to this paper as follows: H.K.: Conceptualization was performed; R.J.: Methodology; M.A.: Data collection; W.T.: Analysis and interpretation of results were conducted; R.H.: Draft manuscript was prepared. All authors reviewed the results and approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| DTCO | = Direct-to-consumer orthodontics |
| ADA | = American Dental Association |
| AAO | = American Association of Orthodontics |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Ethical approval was obtained from the College of Dentistry of Al-Qura University, Saudi Arabia approval No. (HAPO-02-K-012-2023-04-1579).
HUMAN AND ANIMAL RIGHTS
All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committee and with the 1975 Declaration of Helsinki, as revised in 2013.
AVAILABILITY OF DATA AND MATERIALS
The data supporting the findings of the article will be available from the corresponding author [R.H] upon reasonable request.
ACKNOWLEDGEMENTS
Declared none.

