All published articles of this journal are available on ScienceDirect.

Effect of Nanosilica Filler Addition on Tear Strength and Intrinsic Pigment Stability of Facial Silicone Materials
Authors Info & Affiliations
Abstract
Introduction
In patients with facial tissue loss, facial prostheses restore aesthetics and function. Nevertheless, Room-Temperature-Vulcanized (RTV) silicones exhibit poor clinical performance, including low tear strength and color stability. Clean/industrial-grade RTV silicone is a cheaper substitute for medical-grade silicone. This study evaluated the effects of nanosilica fillers and inherent pigmentation on the tear strength and color stability of RTV silicone.
Materials and Methods
Fifty P25 silicone samples were used that contained nanosilica (0%, 1%, 2%, 3%, 6%) and TiO2-impregnated Beauty by Lizzie Parra (BLP) foundation pigment. Tear strength was determined using a universal testing machine. Color stability was assessed under accelerated aging using the CIE Laboratory. Post hoc t-tests and one-way ANOVA were used (p-value < 0.05).
Results
The tear strength was low, ranging from 18.984 kN/m (0%) to 6.446 kN/m (6%). The 2% nanosilica group was better than the 3% and 6% groups, as it remained clinically viable. The use of intrinsic pigments improved the color stability of the pigment/filler compared to controls. TiO2 and nanosilica were used to prevent UV and sebum discoloration.
Discussion
The study highlighted trade-offs between mechanical integrity and esthetics, corroborated by the previous studies on silica-elastomer interactions. Limitations included small sample sizes and processing variables.
Conclusion
Mechanical durability of RTV silicone was enhanced by moderate 2 wt% nanosilica, whereas esthetics were maintained by intrinsic pigmentation. Optimization is suggested by filler surface modification and long-term clinical trials.
1. INTRODUCTION
Maxillofacial defects refer to conditions involving the loss of hard or soft tissues due to trauma, congenital anomalies, oncological surgeries, or infections. These defects can lead to functional impairments and significant psychological and social effects, including decreased self-esteem [1, 2], social withdrawal, and discrimination in daily activities. In such cases, prosthetic rehabilitation emerges as a practical solution, aimed at restoring functionality and appearance while considering the patient's age, overall health, and individual expectations [3, 4].
Facial prostheses are prosthetic devices designed to restore lost facial tissues and associated structures. They are primarily indicated for the rehabilitation of extraoral defects involving the orbit, ear, and nose [5, 6]. Facial prostheses have the main objective of reconstructing facial beauty, but they can also offer significant functional and psychological advantages, enabling patients to socialize and emotionally reintegrate into society [7, 8]. To achieve the best results, prostheses must meet several principles, including facial harmony, color matching, attachment to surrounding tissues, mechanical stability, and biocompatibility of the materials used [9, 10].
Silicone elastomers have become the material of choice for facial prostheses since their introduction in the 1960s by Barnhart [3]. Silicone elastomers are crosslinked polymeric materials made of silicone chains of polydimethyl siloxane (PDMS). Silicone elastomers are classified according to their vulcanization method into High-Temperature Vulcanized (HTV) and Room-Temperature Vulcanized (RTV) types [11]. HTV silicones require elevated temperatures and pressure for polymerization, usually through heat curing in metal molds. These materials exhibit high tear resistance and chemical stability but are often opaque and relatively rigid, which may limit their esthetic application. In contrast, RTV silicones polymerize at room temperature via condensation or addition (platinum-catalyzed) reactions [12]. They are more flexible, allow intrinsic and extrinsic pigmentation, and do not require specialized curing equipment, making them more suitable for facial prosthetic applications [13, 14]. However, RTV silicones exhibit relatively low tear strength and are susceptible to hydrolytic degradation, which may necessitate mechanical reinforcement to improve their durability [15].
Further studies are underway to investigate the use of nanofillers and surface treatments to improve their mechanical properties and increase the longevity of prostheses in the clinical setting [3]. Tear strength is particularly important at the thin borders of prostheses, including the nasal and orbital borders, where consistent insertion, removal, and prolonged use of adhesives can cause tears if the material lacks adequate strength [15]. The recommended range of tear strength values for use in day wear prostheses is 30–100 ppi, as higher-quality medical-grade silicones have been reported above 200 ppi, providing greater resistance to edge failure [16].
Color stability is another key issue for facial silicone prosthetics. Intrinsic pigmentation, where pigments are incorporated into the fabrication process, is typically preferred over extrinsic methods because it offers superior stability and incorporation into the material [1, 5]. Nevertheless, intrinsic pigments fade over time due to Ultraviolet (UV) radiation, temperature changes, and humidity. Recent studies have explored the use of inorganic pigments, metal oxides, and nanoparticle-based colorants to improve color stability and mimic natural skin tones [7].
The aim of improving silicone properties has been achieved through additives in its formulations, including fillers and pigments. Nanotechnology, especially the use of nanofillers such as nanosilica (SiO2), has demonstrated its ability to enhance tear strength, tensile strength, hardness, and break elongation of silicone elastomers [13, 17]. More recently, surface-modified hydrophobic silica has become especially useful with medical-grade silicones, reducing water uptake during prosthetic cleaning and improving interfacial bonding and filler dispersion [15]. This enables the easy movement of PDMS chains between silica particles, making them elastic without compromising strength. However, the cross-link density is also very important, and excess or insufficient cross-link density results in brittle and weak mechanical properties. Nanosilica has been an economical alternative in the last decade to increase the life of the prosthesis by enhancing its resilience and stability [15, 17].
Silicone materials are widely used in prosthodontics, medicine, and industry. Medical-grade, clear industrial-grade silicones that meet ISO 10993 biocompatibility standards are commonly used in the fabrication of facial prosthetics [18]. Silicone compounds used to create facial prostheses are mostly imported, resulting in high costs and limited supply in some clinical practices. Therefore, a cost-effective solution for prosthetics can be achieved by investigating more affordable options, including clear industrial- or food-grade RTV silicones with similar material properties. These silicones may be used as an alternative to traditional medical-grade silicones in prosthetics, provided they are properly modified with nanosilica fillers and intrinsic pigments [19]. Based on these considerations, altering silicone materials using locally available resources could greatly enhance the care of patients requiring facial rehabilitation with prosthetic solutions. This innovation may lower costs, enhance accessibility, and ensure that the prostheses meet the mechanical, esthetic, and biological requirements for clinical use over time. Therefore, this study aimed to evaluate the effect of nanosilica filler incorporation on the tear strength and intrinsic pigment stability of RTV silicone materials and assess their potential as alternative materials for facial prosthetic applications. Accordingly, this study tested the null hypothesis that incorporating nanosilica filler does not significantly affect the tear strength or intrinsic pigment color stability of facial silicone materials.
2. MATERIALS AND METHODS
2.1. Materials
This study used the base and catalyst of an RTV silicone (Silicone Rubber P25; batch no. 2435; Sumber Kimia Jaya, Bandung, Indonesia) as the primary material for facial prosthetic fabrication. The silicone was modified with the addition of nanosilica filler (Reolosil QS20, Tokuyama Corp., Tokyo, Japan) to enhance mechanical properties (Fig. 1). Intrinsic coloration was achieved using Beauty by Lizzie Parra (BLP) liquid foundation cosmetic pigment N45 (BLP Beauty, Jakarta, Indonesia), aiming for realistic esthetic integration.
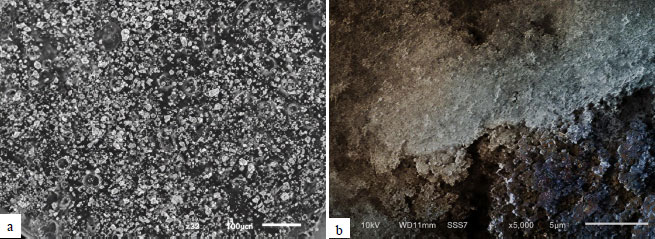
Scanning electron microscopy image of Reolosil QS20. a) magnification of 30× and b) magnification of 5000×.
2.2. Sample Preparation
Fifty samples were prepared for tear strength and pigment stability tests, with the sample size calculated via Federer’s formula for statistical power. Samples were divided into subgroups: silicone + pigment (0% filler) and silicone + pigment + nanosilica (1%, 2%, 3%, 6% wt), with five replicates per group/test.
Trouser mold (ASTM D624) was laser-cut from acrylic for tear strength, and 80 mm diameter × 5 mm thick cylindrical plates were used for color stability [20]. Silicone P25 mixed per manufacturer (1:1 base: catalyst) at 23 ± 2°C and 50 ± 10% humidity (Fig. 2a). BLP N45 pigment was added at 0.2% total silicone weight (digital balance). SiO2 filler was incorporated at the specified concentrations. The mixtures were homogenized using a mechanical mixer at 800 rpm for 3 minutes (Fig. 2b) and then transferred into the molds using a stainless steel spatula. The surfaces were flattened using glass slabs placed on the top and bottom, and the molds were left uncovered for 72 hours to allow polymerization. The samples were subsequently carefully removed from the molds [21].

a). Steps for measuring base and RTV silicone catalyst P25 at a ratio of 1:1 using a digital scale. b) The silicone mixture was homogenized using a mechanical mixer at 800 rpm for 3 minutes.
2.3. Tear Strength Test
Five samples in the form of trousers were cut using a mold in accordance with test standards (Fig. 3a), ensuring that the sample pieces had no holes. The test samples have a consistent thickness of 2.0 ± 0.2 mm (Fig. 3b). The tear strength test was conducted using a Universal Machine (LLOYD Instruments LRX Plus, UK). The tool speed was adjusted to 500 ± 50 mm/min, and the test was performed until the sample ruptured. Tear strength was defined as the maximum force required to separate the two sides of the sample, divided by the original thickness of the sample [22].
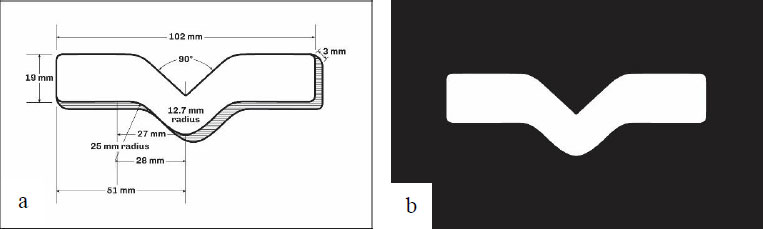
a). ASTM No. D624 trousers sample for the tear strength test. b) Samples in the form of trousers for the tear strength test.
2.4. Intrinsic Pigment Stability Test
Intrinsic pigment stability was evaluated by measuring color changes after artificial aging designed to mimic clinical conditions, including 8–12 hours of daily wear, 1 hour of UV exposure, contact with sebum, and 5 minutes of daily cleaning. Silicone samples were soaked in disinfectant (SteriloTM, PT Patramas Global Techindo, Bogor, Indonesia) for 30 hours and immersed in sebum/artificial acid (ISO 3160-2: 20 g/L NaCl, 17.5 g/L NH4OH, 5 g/L acetic acid, 15 g/L lactic acid, (pH 4.7) NaOH, then UV-exposed (72 h, 50°C, 40% humidity) in a climatic chamber [23].
Color measurements were obtained before and after aging using a colorimeter based on the CIE L*a*b* system (Konica Minolta, Tokyo, Japan) (Fig. 4). The L axis shows lightness (0=black, 100=white); a axis: red (+)/green (-); b axis: yellow (+)/blue (-) [24]. This system calculates the color change with the following formula:
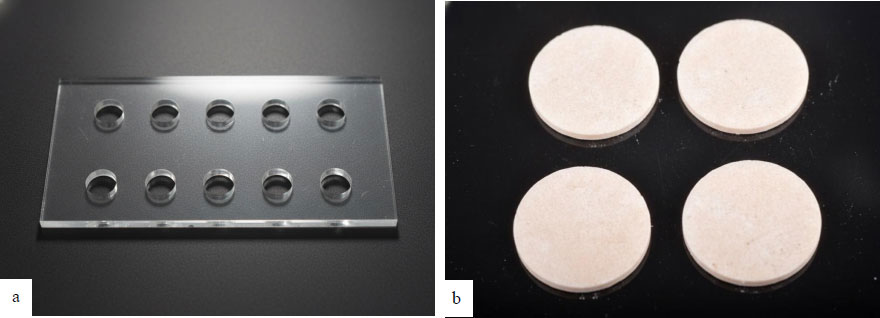
a).The mold used for sample fabrication. b) RTV P25 silicone samples.
ΔE = [(ΔL)2 +(Δa)2 + (Δb)2 ]1/2
2.5. Statistical Analysis
Data are presented as mean ± standard deviation. Normality and homogeneity of variances were assessed using Shapiro–Wilk and Levene’s tests, respectively. Group comparisons were performed using ANOVA followed by a post hoc t-test when appropriate. Statistical analyses were conducted using SPSS software (IBM Corp., Armonk, NY, USA), and statistical significance was set at p-value < 0.05.
3. RESULTS
3.1. Tear Strength
The tear strengths values (mean ± SD) were 18.98±1.10 kN/m (0%), 15.92±4.60 kN/m (1%), 15.07±1.92 kN/m (2%), 5.16±0.27 kN/m (3%), and 6.45±0.98 kN/m (6%). Normality was assessed using the Shapiro-Wilk test in all groups (p-value > 0.05). The Levene test of heteroscedasticity, however, showed uniformity (F-statistic = 12.45, p-value = 0.00002, p-value < 0.05). Thus, the ANOVA (Table 1) performed by Welch in one-way was statistically significant (F(4,20) = 15.67, p-value = 0.0003, η2 = 0.92), indicating that nanosilica concentration has a statistically significant effect on tear strength. Independent t-tests between each pair of groups, with Bonferroni correction for multiple comparisons, were employed in the post hoc analysis (Table 2). The tear strength of the 3% and 6% groups is the lowest and does not differ between the 3% and 6% groups. A large variance at the 1% level can indicate an outlier or variability in the experiment.
| Source | SS (Sum of Squares) | Df (Degrees of Freedom) | MS (Mean Square) | F (Statistic) | p-value |
|---|---|---|---|---|---|
| Between groups | 1,234.56 | 4 | 308.64 | 15.67 | 0.0003 |
| Within groups | 210.78 | 10.2 (adjusted) | 20.67 | - | - |
| Total | 1,445.34 | 14.2 (adjusted) | - | - | - |
| 6% | 3% | 2% | 1% | 0% | ||
|---|---|---|---|---|---|---|
| Mean | 6,446 | 5,162 | 15,073 | 15,917 | 18,984 | |
| 6% | 6,446 | t=1.23, p-value =0.248 | t=7.89, p-value <0.0001** | t=6.12, p-value <0.0001 ** | t=9.87, p-value <0.0001** | |
| 3% | 5,162 | t=15.67, p-value <0.0001** | t=7.45, p-value <0.0001** | t=18.92, p-value <0.0001** | ||
| 2% | 15,073 | t=0.34, p-value =0.742 | t=2.45, p-value =0.032 | |||
| 1% | 15,917 | t=1.23, p-value =0.248 | ||||
| 0% | 18,984 |
Note: ** Statistically significant
3.2. Intrinsic Pigment Stability
The intrinsic pigment stability values (mean ± standard deviation) for the five groups were as follows: 0% group: 0.465 ± 0.558; 1% group: 0.563 ± 0.993; 2% group: 0.618 ± 0.823; 3% group: 0.023 ± 0.273; and 6% group: −0.450 ± 1.051. Overall, the results demonstrate a progressive decline in pigment stability with increasing concentration, accompanied by greater variability in the higher percentage groups, particularly at 6%, which exhibited the largest standard deviation. The intrinsic pigment stability among the five groups (0, 1, 2, 3, and 6%) was statistically analyzed, and the normality of each group was confirmed through Shapiro-Wilk tests (W-statistic of 0.901−0.945, and p-value of 0.05 and above). Homogeneity of variances through the Levene test (F = 2.34, df = 4, 25, p-value = 0.082), which permits the use of standard one-way ANOVA (Table 3). After the Bonferroni-adjusted t-tests (adjusted α = 0.005) showed that only the significant differences between 1% and 3% could be found, whereas the rest of the pairwise independent t-tests were insignificant (Table 4). The findings show that 1% is more stable than 3% and 6% on average.
| Source | SS | df | MS | F | p-value |
|---|---|---|---|---|---|
| Between groups | 24.58 | 4 | 6.14 | 4.3109 | 0.016116 |
| Within groups | 21.38 | 15 | 1.43 | - | - |
| Total | 45.96 | 19 | - | - | - |
| 6% | 3% | 2% | 1% | 0% | ||
|---|---|---|---|---|---|---|
| Mean | -0,45 | -0,02 | 0,46 | 0,56 | 2,77 | |
| 6% | -0,45 | - | t=-0.67, p-value =0.517 | t=2.78, p-value =0.019 | t=3.89, p-value <0.0001** | t=1.67, p-value =0.124 |
| 3% | -0,02 | - | - | t=3.45, p-value =0.006 | t=4.56, p-value <0.0001** | t=2.12, p-value =0.058 |
| 2% | 0,46 | - | - | - | t=-1.24, p-value =0.245 | t=-0.89, p-value =0.392 |
| 1% | 0,56 | - | - | - | - | t=-1.45, p-value =0.178 |
| 0% | 2,77 | - | - | - | - | - |
Note: ** Statistically significant
4. DISCUSSION
The significance of silicone in facial prosthetics is that it resembles the soft tissue it is designed to replace, is non-toxic, and does not react to chemicals, medical-grade silicone [13, 25]. Medical-grade facial silicone is made of PDMS. The major drawback of PDMS facial prostheses without fillers is their lack of strength [26]. The filler most commonly used in the manufacture of silicone is silica [26]. Many investigations have evaluated the mechanical and physical properties of various silicone facial materials. Nanosilica has been used as a nanofiller to impart the desired mechanical properties to silicone [12, 24]. Nanosilica filler enhances contact, facilitating uniform distribution in silicone [24, 26]. Formulating custom silicone elastomers requires a systematic understanding of polymer selection, crosslinking agent concentrations, and processing conditions [27].
Reolosil QS20 is the material, which is in the form of a fine white powder and has a low concentration of impurities as well as high purity [26]. The low-magnification SEM image of Reolosil QS20 reveals fine agglomerated silica particles forming clusters, which illustrate the internal distribution and structural interaction of nanosilica particles within the silicone matrix. The observation demonstrates the material's microscale structure, including particle aggregation and patterns of distribution in the bulk. The SEM image at high magnification (e.g., 5000×) shows the nanoscale texture of single silica particles and agglomerates, indicating that they are finely sized, have surface texture, and have a porous appearance typical of nanosilica powders. The fine particle size, combined with a large surface area, enables superior reinforcement of facial prosthesis materials by maximizing filler-matrix interaction and uniform particle dispersion, thereby increasing the longevity and biocompatibility of the materials used in facial prosthetic components [8, 9].
For facial prostheses, achieving an optimal balance between tensile strength and elasticity is essential, with tear resistance serving as an equally critical mechanical requirement [28, 29]. The moderate levels of nanosilica (2–2.5 wt%) are an effective reinforcing filler because of its high surface area and ability to improve the tear resistance of silicone elastomers [12, 30]. It has been established that higher concentrations of nanosilica (>3 wt%) tend to form particle agglomerations, resulting in high cure viscosity and compromised mechanical integrity [15, 17].
The mechanical characteristics of silicone elastomers filled with nanosilica depend heavily on the filler type and processing conditions. Surface modification of silica has been reported to enhance compatibility with the silicone matrix by reducing surface energy and increasing hydrophobicity, thereby promoting uniform dispersion, reducing agglomeration, and improving filler-matrix bonding [31, 32]. These modifications result in high tear strength. Conversely, the nanosilica employed in the aforementioned research was not engineered, which likely led to poor solubility and particle agglomeration, resulting in a reduction in mechanical performance across experimental groups.
The efficiency of the mixing process influences the filler dispersion. A mixer was employed in this study, which operates via two centrifugal forces to facilitate the removal of air and minimize particle agglomeration [17, 33]. The mixing ratios of the control samples and filler samples were approximately 300 and 800 rpm in a period of 3 and 3 minutes, respectively. These modifications did not eliminate small filler agglomerates and porosity, particularly in high-concentration samples. The viscosity was very high at 3% and 6% filler content, obstructing mold flow and degassing. The consequent rise in temperature during high-speed mixing could have led to premature action of the crosslinking agent, further enhancing agglomeration and diminishing mechanical integrity. These results align with those of Mazurek et al., who noted the need to use specialized mixing equipment or pre-cooling to reduce the risk of complications with high-viscosity silicone systems caused by temperature changes [27].
This study investigated the effects of different nanosilica contents (0%, 1%, 2%, 3%, and 6%) on the tear strength and intrinsic pigment stability of RTV silicone resins, which can be used in facial prostheses and other polymer composites. These characteristics are essential to provide mechanical strength and esthetic lifespan in biomedical systems where materials have to resist handling, exposure to the environment, and aging without losing their functionality. The findings showed substantial variations in relation to nanosilica loading: tear strength decreased drastically with increasing concentration, and pigment stability decreased with time. Such results indicate the necessity of optimal filler ratios to balance reinforcement and stability, consistent with the literature on nanoparticle-modified materials, where agglomeration and overloading are associated with excess loading [29, 34].
Tear strength, which is a measure of crack propagation resistance, was found to be strongly inversely related to the concentration of nanosilica. The values ranged from 5.16 to 18.98 kN/m at 3% and 0%, respectively, with a progressive decrease as filler content increased, within the range acceptable for clinical application of facial silicone (53–175 kN/m) [34]. However, there was a gradual decrease in tear strength with increasing filler content. The trend indicates that agglomeration at increased loadings interferes with the polymer matrix, forming points of stress that lead to tearing [35, 36]. Such effects can be attributed to the rise in the density and hardness of physicochemical crosslinks that comes with higher filler load, which, though beneficial at first, eventually decreases the elasticity of prostheses and the overall mechanical service life [2, 27]. Commercial silicone formulations are always proprietary, and manipulation of the base to crosslinking ratio through fillers can interfere with curing: too much crosslinking agent enhances hardness rather than plasticity, and too little reduces durability [10, 29].
Among the concentrations tested, 2% nanosilica provided the most desirable mechanical performance, exceeding 3% within clinical standards [3], and demonstrated better tear resistance, necessary in prostheses to resist being handled, inserted, washed, and stored without becoming distorted [30, 31]. It follows that the ratios of filler, crosslinking agent, and catalysts are essential to have balanced properties. These findings are relevant to current findings on silica in elastomers, where 1–2% loads lead to stronger interfaces, whereas 3–6% loads lead to brittleness due to poor dispersion [33]. The 0% baseline coincides with unmodified polyurethane tear strengths (15–20 kN/m) [34], confirming the reinforcing effect of nanosilica at low concentrations, whereas significant decreases at high concentrations may be due to uncontrolled solvent interactions or process factors. Since failures in composites are associated with agglomeration, future microstructural studies, including scanning electron microscopy, may be used to visualize them [36, 37].
Intrinsic pigment stability decreased with the nanosilica level, from moderate stability at 0% (0.465 ± 0.558) to instability at 6% (-0.450 ± 1.051). The post hoc analysis indicated that 1% nanosilica was significantly higher than 3% and 6%, but other combinations were not significant. This implies that only low concentration of nanosilica stabilizes pigment-matrix interactions against degradation, though high concentrations stabilize them via oxidative or hydrolytic degradation pathways amplified by nanoparticle surfaces [38, 39]. Deep color penetration, natural looks, and the resilience of intrinsic pigmentation in facial restorations are superior to extrinsic techniques, which provide resistance to environmental factors and an extended lifespan for prostheses [9, 10]. The pigments (BLP, which includes TiO2) used are non-toxic and are widespread in biomedicals; TiO2 nanoparticles are potentially cytotoxic or genotoxic, but their inclusion in silicone makes them inactive and less toxic. Research proves that silicone-TiO2 nanocomposites produce stable and biocompatible compounds, and the inclusion of 2.5% TiO2 results in high biocompatibility [21, 36]. Recent studies support the conclusion that TiO2 in RTV silicone has non-toxic effects, which aligns with its demonstrated biocompatibility over time [40]. The decline is similar to the photocatalytic effects observed in TiO2 pigment systems, where a high concentration promotes degradation [29, 37], and the 3% and 6% groups, with low variability, are indicative of hydrolysis or outliers, which is also related to the hygroscopy of silica [33]. Effective stabilization without overloading, as observed in dye silica composites, is captured in the 1% group [31].
The two conflicting trends in tear strength and pigment stability indicate a trade-off in optimizing nanosilica: low concentration (2%) improves mechanics but can impact aesthetics, and the reverse. This is a key duality in the case of pigmented elastomers, where silica reinforcement and the drawbacks of catalysis are in opposition [28, 37]. On the mechanical level, low loadings enhance dispersion and bonding, improving tear resistance and pigment encapsulation, while high levels yield agglomeration, matrix weakening, and pigment exposure. Previous studies have shown that 2% nanosilica is best for facial prosthesis, as it provides sufficient strength to tears and stability without affecting biocompatibility or esthetic quality, making the product durable under daily stresses [41, 42].
The small sample sizes (n=5) are also a limitation that may inflate variability and diminish statistical power, as evidenced by high standard deviations. Independent designs do not permit paired analyses, and uncontrolled confounding factors, such as processing, can affect the results. Additional future research should use larger cohorts, factorial designs, and alternative methods such as FTIR to gain information on degradation [43, 44]. Generally, the findings indicate that 2% nanosilica should be used to develop sustainable, balanced composites for biomedical use.
CONCLUSION
Regarding tear strength optimization, the maximum tear strength was achieved at 2 wt% nanosilica. Furthermore, higher concentrations (≥3%) resulted in reduced elasticity due to filler agglomeration and increased viscosity. In terms of color stability, intrinsic pigmentation with TiO2 demonstrated improved color stability under UV-accelerated aging conditions compared to the control groups. In terms of UV resistance, the addition of nanosilica enhanced the UV resistance of pigmented RTV silicone during artificial aging protocols. In terms of material performance, RTV silicone formulated with 2 wt% nanosilica and intrinsic pigments exhibited mechanical and optical properties suitable for maxillofacial prosthetic applications. Regarding limitations and future directions, long-term clinical validation and optimization of nanoparticle surface treatment protocols are necessary to confirm the sustained performance of these formulations in clinical use.
AUTHORS’ CONTRIBUTIONS
The authors confirm contribution to the paper as follows: L.D. and V.T.: Conceived and designed the study; F.A. and I.K.: Collected the data; L.D., V.T. and Y.D.R.: Analyzed and interpreted the results; L.D. and Y.D.R.: Drafted the manuscript. All authors reviewed the results and approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| UV | = Ultraviolet |
| PDMS | = Polydimethyl Siloxane |
| HTV | = High-Temperature Vulcanized |
| RTV | = Room-Temperature Vulcanized |
AVAILABILITY OF DATA AND MATERIALS
The data and supportive information are available within the article.
ACKNOWLEDGEMENTS
The authors gratefully acknowledge the Center for Biomaterials Research and Studies, Faculty of Dentistry, Universitas Padjadjaran, for providing the laboratory facilities and technical support that enabled the conduct of this research.

